





The most powerful testosterone intervention available to most men costs nothing, requires no prescription, and is available every single night. Most men are not using it correctly.
Sleep is not recovery. That framing undersells it by about a factor of ten. Sleep is the primary hormonal manufacturing window in the male body. It is when the majority of daily testosterone is produced, when growth hormone peaks, when cortisol resets, and when the entire neuroendocrine system runs its maintenance cycle. Treating it as the thing you do after everything else is done is one of the more expensive mistakes a man can make with his health, and I mean that in a biochemical sense, not a philosophical one.
I spent a long time prioritizing supplements over sleep. I was the person researching herbal extracts at midnight on a phone screen, optimizing a stack for hormonal support while actively destroying the hormonal environment those supplements were supposed to help. It took an embarrassingly long time to recognize the contradiction.
If you have been building out a broader approach to hormonal health, the complete guide to natural testosterone support makes clear that sleep is not a secondary recommendation. It is the foundation everything else is built on.
What actually happens to testosterone while you sleep
Testosterone secretion follows a predictable daily rhythm called a circadian pattern. Levels begin rising in the early hours of the morning, peak shortly after waking, and decline gradually through the afternoon and evening. That morning peak does not come from nowhere. It is built during the night, primarily during slow-wave sleep and REM stages, through a series of hormonal pulses orchestrated by the hypothalamus and pituitary gland.
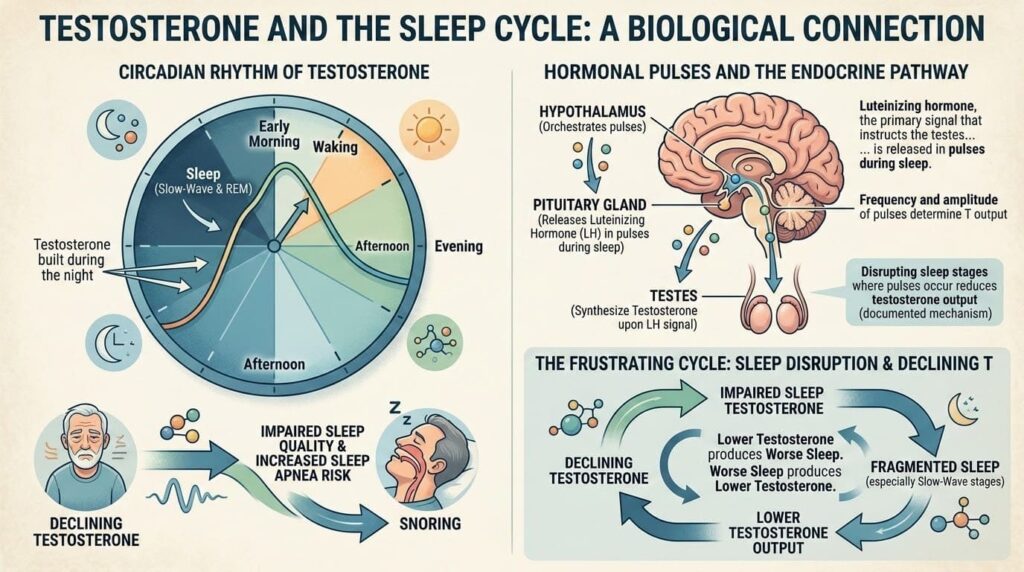
Luteinizing hormone, the primary signal that instructs the testes to synthesize testosterone, is released in pulses during sleep. The frequency and amplitude of those pulses determine how much testosterone is available the following morning. Disrupt the sleep stages where those pulses occur most densely, and you directly reduce testosterone output. This is not a hypothesis. It is a documented mechanism with a clear physiological chain of causation.
The relationship also runs in the other direction, which is what makes this a particularly frustrating cycle for men dealing with both issues simultaneously. Declining testosterone impairs sleep quality and increases susceptibility to sleep-disordered breathing, including obstructive sleep apnea. Sleep apnea fragments sleep architecture precisely in the slow-wave stages where testosterone secretion is highest. Lower testosterone produces worse sleep. Worse sleep produces lower testosterone. Round and round.
The University of Chicago study that should have changed everything
In 2011, researchers at the University of Chicago published a study in the Journal of the American Medical Association that deserves far more mainstream attention than it received. They took a group of healthy young men, average age 24, with no sleep disorders or hormonal issues, and restricted their sleep to five hours per night for one week. Daytime testosterone levels fell by 10 to 15% compared to their own fully-rested baseline.
That decline happened in one week. In healthy young men at peak hormonal age.
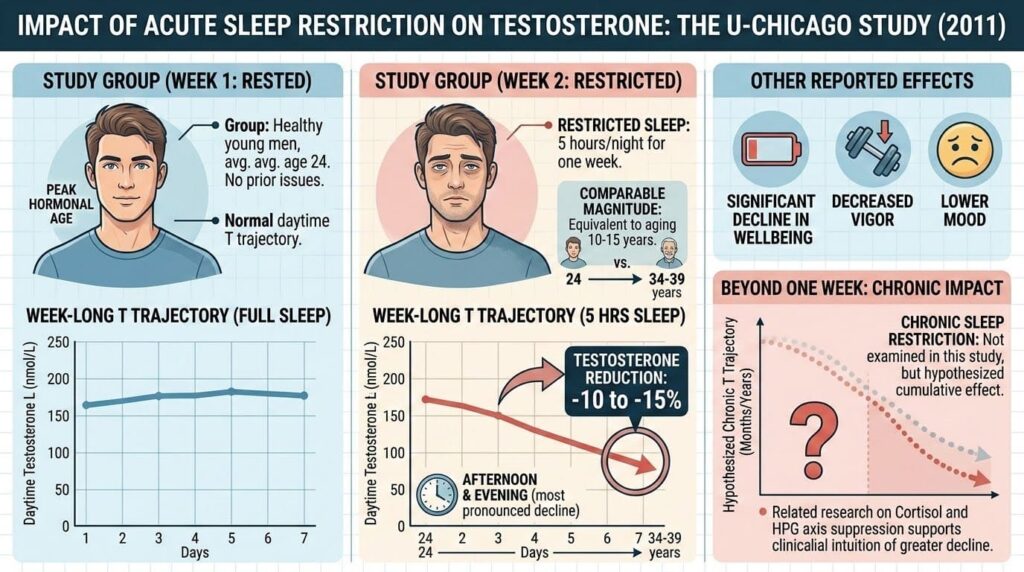
That study put numbers on something clinicians had suspected for years: sleep restriction produces testosterone suppression that is rapid, measurable, and comparable in magnitude to the hormonal change associated with aging ten to fifteen years. The effect appeared most pronounced in the afternoon and early evening hours, which aligns with the timing of when sleep-built testosterone reserves are being drawn down.
The researchers noted that the men also reported significant declines in wellbeing, vigor, and mood over the same period. These were not subtle background changes. They were noticeable within days.
What that study did not examine, because it was not designed to, is what chronic partial sleep restriction across months and years does to testosterone trajectories. The clinical intuition, supported by related research on cortisol and HPG axis suppression, is that the cumulative effect is considerably more significant than any one-week snapshot captures.
Why five hours feels fine until it does not
One of the most consistent findings in sleep restriction research is that people adapt subjectively to reduced sleep far faster than their physiology does. After a few nights of short sleep, the feeling of sleepiness diminishes. People report feeling adjusted. Their performance on objective cognitive and hormonal tests continues to decline.
This is the quiet danger of chronic sleep restriction. The feedback mechanism that normally signals the need for more sleep becomes blunted. A man running on six hours for months may genuinely feel functional while his testosterone, cognitive performance, and metabolic health are measurably compromised compared to his own well-rested baseline.
The reference point shifts. He stops remembering what feeling genuinely rested and hormonally replete feels like, so the gap becomes invisible.
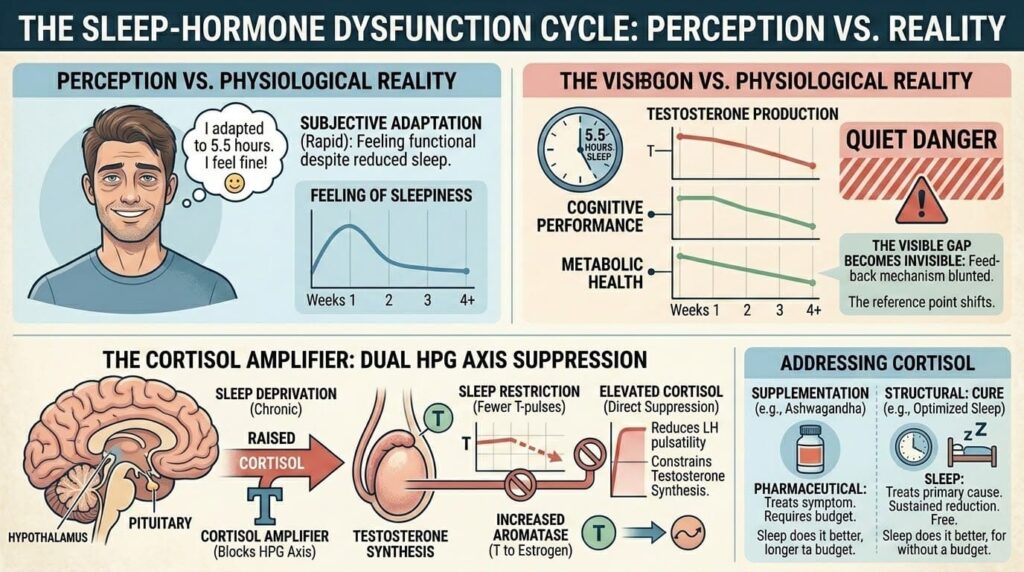
The cortisol amplifier
Sleep deprivation does not only reduce testosterone by shortening the hormonal manufacturing window. It also raises cortisol, and elevated cortisol suppresses the HPG axis directly. The two mechanisms compound each other in a way that makes the total hormonal impact of poor sleep considerably larger than either pathway alone would suggest.
A single night of poor sleep elevates cortisol the following morning. Sustained poor sleep keeps cortisol chronically elevated. Chronically elevated cortisol reduces LH pulsatility, constrains testosterone synthesis, and increases the activity of aromatase, the enzyme that converts testosterone to estrogen. The man who is supplementing with adaptogens to lower cortisol while continuing to sleep five to six hours is treating a symptom while maintaining the primary cause.
This is why the conversation about ashwagandha, one of the most evidence-supported herbs for cortisol reduction, belongs in the same breath as sleep. Both address cortisol. One does it pharmaceutically, the other structurally. Sleep does it better, for longer, and without a supplement budget.
What the research says about sleep quality vs. sleep duration?
Duration and quality are related but distinct variables, and research increasingly suggests that quality may be the more important of the two for hormonal outcomes specifically.
| Sleep Variable | Hormonal Relevance | Key Research Finding |
| Total duration under 6 hrs | Significant testosterone reduction | 10-15% drop in one week (UChicago, 2011) |
| Slow-wave sleep disruption | Reduced LH pulsatility | Direct suppression of testosterone synthesis |
| REM fragmentation | Elevated cortisol | Secondary HPG axis suppression |
| Sleep apnea | Compounded effect | Fragments SWS and REM simultaneously |
| Consistent wake time | Circadian hormone alignment | Anchors morning testosterone peak |
A man sleeping seven hours with frequent arousals, light-stage dominance, and no deep sleep may have worse hormonal outcomes than a man sleeping six and a half hours of genuinely consolidated, deep sleep. This is relevant because many sleep interventions focus on time in bed rather than architecture, and the two are not the same thing.
Alcohol is the most common disruptor of sleep architecture that people consistently underestimate. Even moderate consumption within three hours of sleep suppresses slow-wave sleep, fragments REM, and elevates nighttime cortisol. The sleep that follows alcohol feels like rest because loss of consciousness feels like rest. The hormonal output of that night does not reflect rest.
Practical strategies with actual research support
Room temperature is one of the most reliably actionable variables in sleep quality research. Core body temperature must drop to initiate and maintain deep sleep. A bedroom cooled to somewhere between 65 and 68 degrees Fahrenheit supports that process. This is not a wellness trend. It is thermoregulation physiology.
Morning light exposure within the first thirty to sixty minutes of waking is the most potent natural circadian signal available. Bright outdoor light suppresses residual melatonin, elevates morning cortisol appropriately, and sets the timing of the evening melatonin rise that facilitates falling asleep. This single habit, done consistently, does more for circadian alignment than most sleep supplements combined.
Consistent wake time, maintained even on weekends, anchors the circadian rhythm more effectively than consistent bedtime does. Sleep timing research consistently finds that social jet lag, the shift in sleep timing between weekdays and weekends, fragments circadian rhythm in ways that measurably affect hormonal output across the week.
Blue light from screens in the two hours before bed competes with the melatonin signal. The effect is real but has been somewhat overstated. Screen brightness and proximity matter more than blue light content specifically. Dimming screens and holding them further from the face produces a meaningful reduction in circadian disruption without requiring blue-light glasses or total abstinence from evening device use.
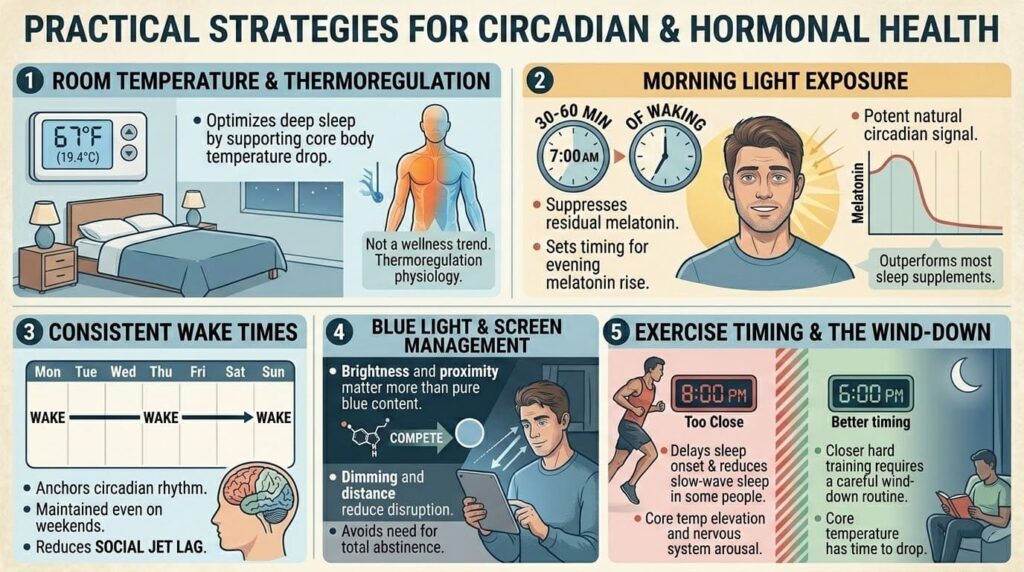
Exercise timing is worth mentioning because it is frequently misunderstood. High-intensity training within two to three hours of sleep can delay sleep onset and reduce slow-wave sleep in some people, not through cortisol alone but through core temperature elevation and nervous system arousal. This does not mean avoiding evening training. It means recognizing that the closer hard training is to bedtime, the more careful the wind-down routine needs to be.
The supplement stack built on a broken foundation
There is a particular kind of irony in a man who researches zinc, tongkat ali, and vitamin D with genuine seriousness, spending real money on high-quality standardized extracts, and then sleeps six hours a night on a phone-lit schedule with two glasses of wine before bed.
Every supplement in that stack is operating in a hormonally suppressed environment created by the sleep habits. The zinc is present. The aromatase inhibition is happening. The HPG axis stimulation from the herbal extract is occurring. But the system those interventions are trying to support is simultaneously being suppressed by chronically elevated cortisol and truncated testosterone synthesis windows.
Understanding zinc’s foundational role in the testosterone production pathway matters. So does understanding that all of it operates downstream of the hormonal environment created by sleep. Fix the foundation, and the supplements work better. Ignore the foundation, and the supplements are fighting upstream against a problem they were never designed to solve.
The most honest recommendation in male hormonal health in 2026 is also the least commercially exciting one: before spending another dollar on a new supplement, spend thirty days taking sleep seriously as a primary intervention. Set a consistent wake time. Cool the room. Cut alcohol within three hours of sleep. Get morning light. Track how you feel in weeks three and four compared to week one.
The results will be more convincing than most clinical trials on the supplements currently sitting in your cabinet.
The question that follows from all of this is worth sitting with: if seven to nine hours of quality sleep produces hormonal changes comparable in magnitude to some of the most significant supplement findings in the research literature, why does it remain the most consistently underused tool in men’s health?