





Most men think they understand vitamin D. Sunlight is the source, they know that much. Bone health and immune function get a mention too, somewhere in the back of their minds. Somewhere in their bathroom cabinet sits a bottle of it, taken inconsistently, at a dose that felt reasonable when they bought it. What most men do not know is that vitamin D is not really a vitamin at all, and that the distinction changes everything about how it relates to testosterone.
Calling vitamin D a vitamin is one of the more consequential mislabelings in nutritional science. It is synthesized in the skin from cholesterol in response to ultraviolet B radiation, transported to the liver and kidneys for conversion into its active form, and then distributed to receptor sites in virtually every tissue in the human body. That is not a vitamin. That is a hormone. A prohormone, more precisely, and one with a direct line into the biological machinery that produces testosterone.
I find this one of the more fascinating intersections in nutritional medicine, partly because it has been sitting in the research literature for well over a decade and still somehow remains on the periphery of how most men think about their hormonal health. The conversation about natural testosterone support tends to gravitate toward exotic herbs and complex protocols. Vitamin D is neither exotic nor complex. It is also, for a remarkable percentage of American men, simply missing.
The prohormone distinction and why it matters
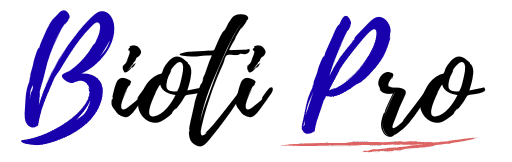
The active form of vitamin D, calcitriol, binds to vitamin D receptors (VDRs) distributed throughout the body. These receptors are not incidental. They are present in the brain, the immune system, the cardiovascular system, and critically for this conversation, in the Leydig cells of the testes. Leydig cells are the specialized cells responsible for producing testosterone in response to luteinizing hormone signals. The fact that they carry vitamin D receptors is not a footnote. It is a direct structural link between vitamin D status and testosterone synthesis capacity.
Research has identified vitamin D response elements in the promoter regions of genes involved in steroidogenesis, which is the biological process of converting cholesterol into steroid hormones including testosterone. This means vitamin D does not merely correlate with testosterone levels in some indirect or incidental way. It appears to directly regulate gene expression in testosterone-producing cells.
That is a mechanistic connection. It is specific, it is documented, and it gives the clinical research findings a coherent biological framework to rest on.
What the clinical evidence shows
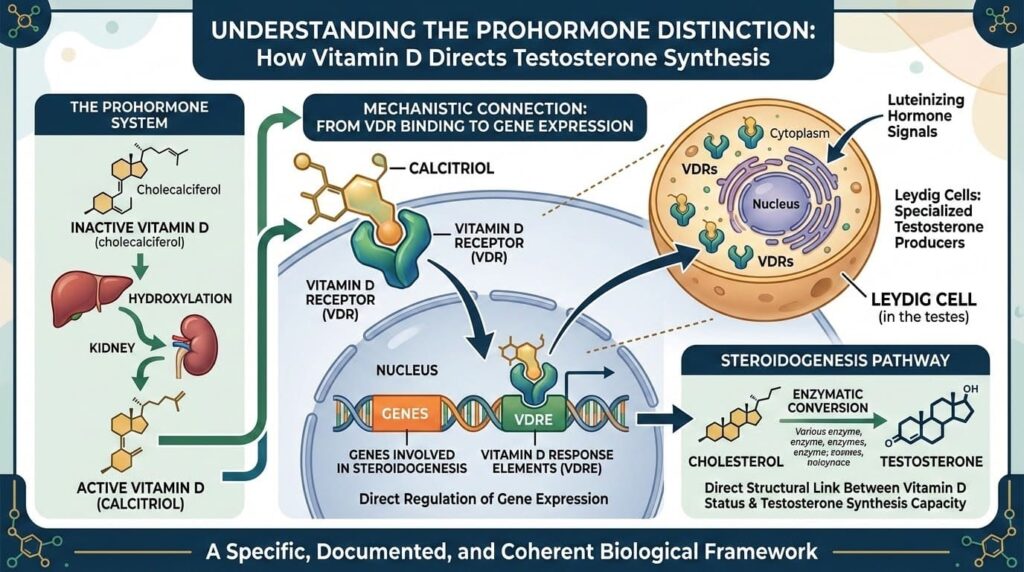
The most cited randomized controlled trial on this specific question was published in Hormone and Metabolic Research in 2011. Researchers at the Medical University of Graz in Austria assigned 165 overweight but otherwise healthy men to receive either 3,332 IU of vitamin D daily or a placebo for twelve months. Men in the vitamin D group showed significantly higher total testosterone, free testosterone, and bioactive testosterone at the end of the trial compared to both their own baseline and the placebo group.
That study is notable for several reasons. It used a meaningful dose over a meaningful duration. It measured multiple testosterone fractions, not just total testosterone. And the effect size was clinically relevant, not merely statistically detectable on a large enough sample.
Observational research has consistently extended that picture. A large cross-sectional study using data from the European Male Aging Study found a significant positive correlation between serum 25-hydroxyvitamin D levels and testosterone across a broad age range. Men with higher vitamin D status consistently showed higher testosterone values, and the relationship held after controlling for factors including age, body mass index, physical activity, and season of testing.
A 2023 meta-analysis published in Nutrients compiled data from multiple intervention trials and concluded that vitamin D supplementation produced statistically significant increases in total testosterone in men who were vitamin D insufficient at baseline. The effect was more modest or absent in men who were already vitamin D sufficient, which mirrors the pattern seen with zinc and suggests the hormone-optimization benefit operates through deficiency correction rather than supraphysiological loading.
How widespread is the deficiency problem
The short answer is: more widespread than most men realize, and geographically skewed in ways that catch people off guard.
Vitamin D synthesis requires ultraviolet B radiation at a specific wavelength. That wavelength is only present in sufficient intensity when the sun is at a high enough angle in the sky, a condition that varies dramatically by latitude and season. Men living above approximately 37 degrees north latitude, which includes most of the United States north of Richmond, Virginia and the California central coast, produce virtually no vitamin D from sun exposure between November and March regardless of time spent outdoors.
Add indoor work schedules, sunscreen use, darker skin pigmentation that reduces UV absorption, and increasing amounts of time spent in climate-controlled environments, and the result is a population with structurally inadequate sun exposure for vitamin D synthesis across large portions of the year.
| Risk Factor | Mechanism | Affected Population |
| Northern latitude residence | Insufficient UVB angle in winter | Most of continental US above 37N |
| Indoor occupation | Limited daily sun exposure | Office workers, remote workers |
| Darker skin pigmentation | Higher melanin reduces UV absorption | Men of African, South Asian, Hispanic descent |
| Obesity | Vitamin D sequestered in adipose tissue | Men with BMI over 30 |
| Age over 50 | Reduced skin synthesis efficiency | Older adult men |
| Chronic kidney or liver disease | Impaired conversion to active form | Men with metabolic conditions |
The National Health and Nutrition Examination Survey data consistently estimates that somewhere between 40 and 70 percent of American adults have insufficient vitamin D status, depending on the threshold used. Among men with multiple risk factors from the table above, that number climbs considerably higher.
Obesity deserves specific attention here because it creates a particularly compounding problem. Adipose tissue sequesters vitamin D, making it less bioavailable. Obesity is also independently associated with lower testosterone through elevated aromatase activity in fat tissue. A man who is overweight, works indoors, and lives in Chicago in February is facing a genuinely significant vitamin D deficit, and the hormonal consequences of that deficit are layering onto other mechanisms already working against his testosterone levels.
Understanding your numbers
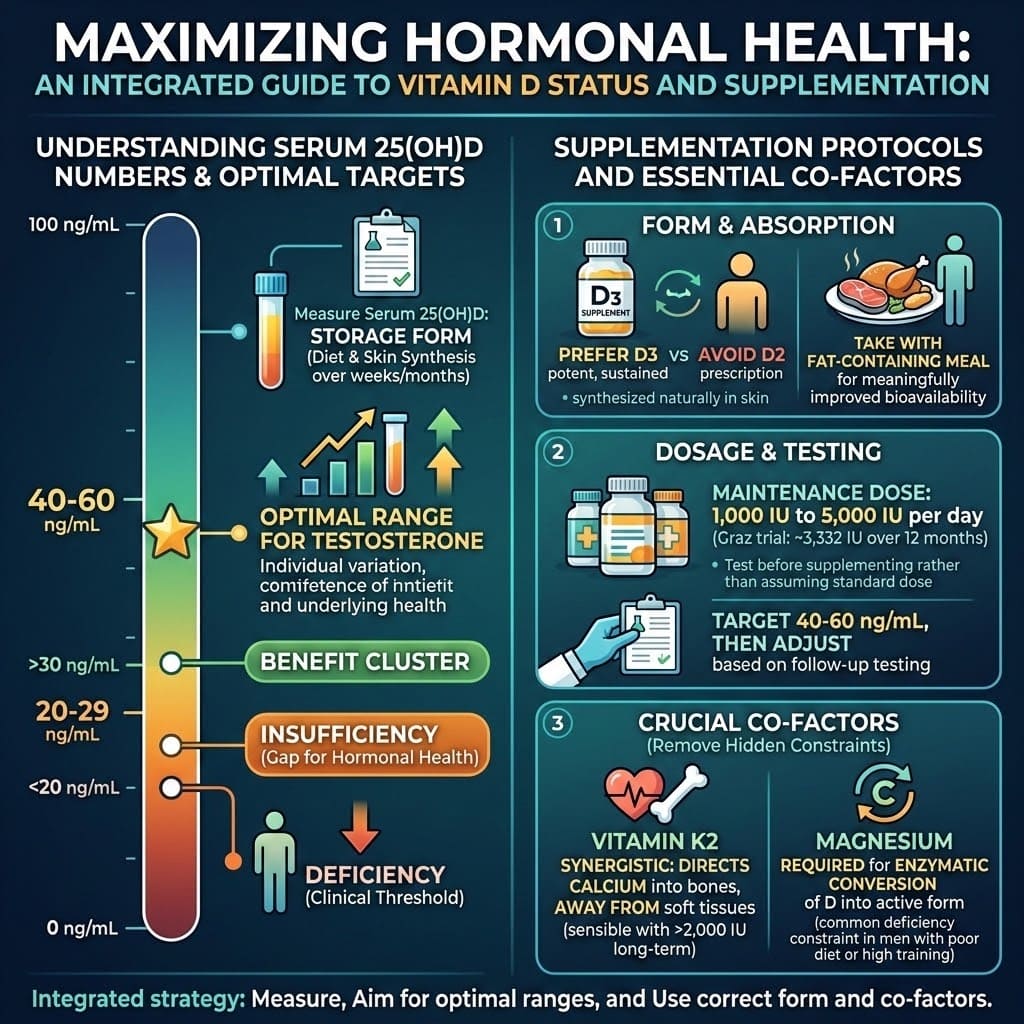
The standard blood test for vitamin D status measures serum 25-hydroxyvitamin D, written as 25(OH)D. This is the storage form, and it reflects both dietary intake and skin synthesis over the preceding weeks and months.
The conventional medical threshold for deficiency is below 20 ng/mL. Insufficiency is typically defined as 20 to 29 ng/mL. But the research on testosterone and hormonal health generally clusters its positive findings in populations with levels above 30 ng/mL, with some studies suggesting that the hormonal benefits plateau somewhere between 50 and 80 ng/mL.
This creates a practical gap. A man with a 25(OH)D of 22 ng/mL is technically not deficient by clinical standards. He is also not operating in the range where the testosterone research shows meaningful hormonal benefit. Aiming for a level between 40 and 60 ng/mL is a reasonable target for men prioritizing hormonal health, though individual variation and underlying health status should inform where exactly within that range makes sense.
Testing is straightforward. It is included in many standard annual blood panels, and standalone vitamin D testing is widely available and inexpensive. Given how common insufficiency is and how significant the hormonal implications are, testing before supplementing is genuinely worth doing rather than simply assuming a standard dose will land you in an optimal range.
Supplementation: getting the dose and form right
Vitamin D3, the form synthesized naturally in human skin, is the preferred supplemental form. Vitamin D2, sometimes used in prescription formulations, is less potent on a per-milligram basis and produces lower and less sustained blood levels. When buying a supplement, D3 is the one to reach for without exception.
Vitamin D is fat-soluble, meaning it requires dietary fat for absorption. Taking a D3 supplement with a meal that contains some fat, even a small amount, meaningfully improves bioavailability compared to taking it on an empty stomach or with a fat-free meal.
Dose ranges in the research range widely, from around 1,000 IU to 5,000 IU per day for maintenance in adults. The 2011 Graz trial used approximately 3,332 IU and produced significant testosterone-relevant results over twelve months. Most functional medicine practitioners working in hormonal health target supplementation doses that bring 25(OH)D into the 40 to 60 ng/mL range and then adjust based on follow-up testing rather than applying a fixed dose universally.
One important co-factor worth knowing: vitamin K2 works synergistically with vitamin D3 by directing calcium into bones and away from soft tissues. Long-term high-dose vitamin D supplementation without adequate K2 can potentially drive calcium deposition in arterial walls. This does not mean vitamin D is dangerous. It means pairing D3 with K2 in a combined formula or separate supplement is a sensible practice for anyone supplementing at 2,000 IU or above on an ongoing basis.
Magnesium also deserves mention. It is required for the enzymatic conversion of vitamin D into its active form, and magnesium deficiency is common in men with poor diets or high training volumes. A man who is magnesium-depleted may supplement vitamin D adequately yet still see limited increases in active calcitriol because the conversion enzyme lacks its required cofactor. Ensuring adequate magnesium intake, through food or supplementation, removes that hidden constraint.
Where vitamin D fits in the broader picture
Vitamin D does not operate in hormonal isolation any more than zinc or sleep does. It sits within the same interconnected system that all of the other testosterone-relevant interventions address from different angles.
Consider the convergence: vitamin D supports Leydig cell function and steroidogenesis directly. Zinc acts as a cofactor in the same steroidogenesis pathway and moderates aromatase. Ashwagandha reduces the cortisol load that suppresses the HPG axis upstream. Sleep provides the temporal window in which the HPG axis actually executes testosterone production. Each of these addresses a distinct point of leverage within the same system.
What makes vitamin D particularly worth prioritizing is that its deficiency is structural rather than behavioral for many men. A man who manages his stress, sleeps adequately, and eats well can still be vitamin D insufficient simply by virtue of where he lives and how modern life is structured. That is a correctable problem with a straightforward intervention, a point in its favor that does not require any lifestyle overhaul.
The practical step most men skip is the blood test. They assume either that they are fine or that a standard 1,000 IU supplement covers the gap, and they never actually verify either assumption. Given that the research on vitamin D and testosterone consistently shows the benefit concentrating in men who are insufficient at baseline, knowing your number is not optional context. It is the starting point.
Understanding how sleep architecture governs the hormonal window in which all of these nutrients do their work adds the final dimension to a complete picture. Vitamin D enables the production machinery. Sleep provides the operating schedule. Both need to be addressed before layering in herbs, adaptogens, and more targeted interventions.
The research on vitamin D and testosterone is not emerging science. It is a decade-plus body of evidence with a coherent mechanism, a clear deficiency problem in the target population, and a low-risk, low-cost solution. The more interesting question is why it consistently gets less attention than supplements that cost ten times as much and have a fraction of the human trial data behind them.