





The medication changed everything about eating except the need to eat well. Appetite vanished. Portions shrank to fractions of their former size. Food that once brought pleasure became functional at best and nauseating at worst. And somewhere in this dramatic transformation, millions of Americans taking Ozempic, Wegovy, Mounjaro, and similar GLP-1 medications face a question their prescribers rarely answer adequately: how exactly should I eat now?
The weight is coming off. That part works as advertised. But what kind of weight? Clinical trials reveal that up to 39% of weight lost on GLP-1 therapy comes from lean muscle mass rather than fat. Hair falls out. Energy crashes. Nutrient deficiencies develop silently. The scale celebrates while the body quietly struggles.
This disconnect between pharmaceutical success and nutritional neglect represents one of the most significant gaps in modern weight management care. GLP-1 medications have revolutionized obesity treatment, with the market now exceeding $50 billion annually and prescriptions reaching record levels through 2026. Yet the conversation around these medications focuses almost exclusively on pounds lost rather than health preserved.
Eating well on GLP-1 therapy requires abandoning conventional nutrition wisdom and rebuilding from fundamentally different principles. When you can only consume 1,000 to 1,200 calories daily, every bite carries weight that normal eating never demanded. A digestive system operating at half speed also means food choices that once seemed reasonable can become intolerable. On top of that, when appetite centers in the brain no longer signal appropriately, external structure must replace internal cues.
This GLP-1 nutrition guide provides the framework for navigating these challenges. Not generic weight loss advice repackaged for a new medication class, but specific strategies addressing the unique physiological changes these drugs produce. The goal extends beyond weight loss to encompass what matters more: arriving at a lower weight with preserved muscle, adequate nutrition, sustained energy, and the foundation for long-term maintenance.
The medication handles appetite. Everything else remains your responsibility.
GLP-1 receptor agonists are a class of injectable medications originally developed to treat type 2 diabetes. They mimic glucagon-like peptide-1, a natural hormone that regulates blood sugar, slows gastric emptying, and signals fullness to the brain.
Because they significantly reduce appetite, several GLP-1 medications are now FDA-approved for chronic weight management in adults with obesity or overweight with related health conditions.
Common examples: Ozempic and Wegovy (semaglutide), Mounjaro and Zepbound (tirzepatide), Saxenda (liraglutide), and Trulicity (dulaglutide).
How GLP-1 medications transform digestion and appetite
Understanding what these medications actually do to your body explains why eating changes so dramatically and why certain strategies succeed while others fail.
GLP-1 stands for glucagon-like peptide-1, a hormone naturally produced in the intestines after eating. Under normal circumstances, GLP-1 stimulates insulin release, suppresses glucagon, slows gastric emptying, and signals satiety to the brain. The problem is that natural GLP-1 breaks down within minutes. Its effects are fleeting.
Medications like semaglutide and tirzepatide are modified versions that resist breakdown. A single weekly injection maintains elevated GLP-1 activity for days rather than minutes. The effects that normally last briefly after meals become continuous, producing the dramatic appetite suppression these medications have become famous for.
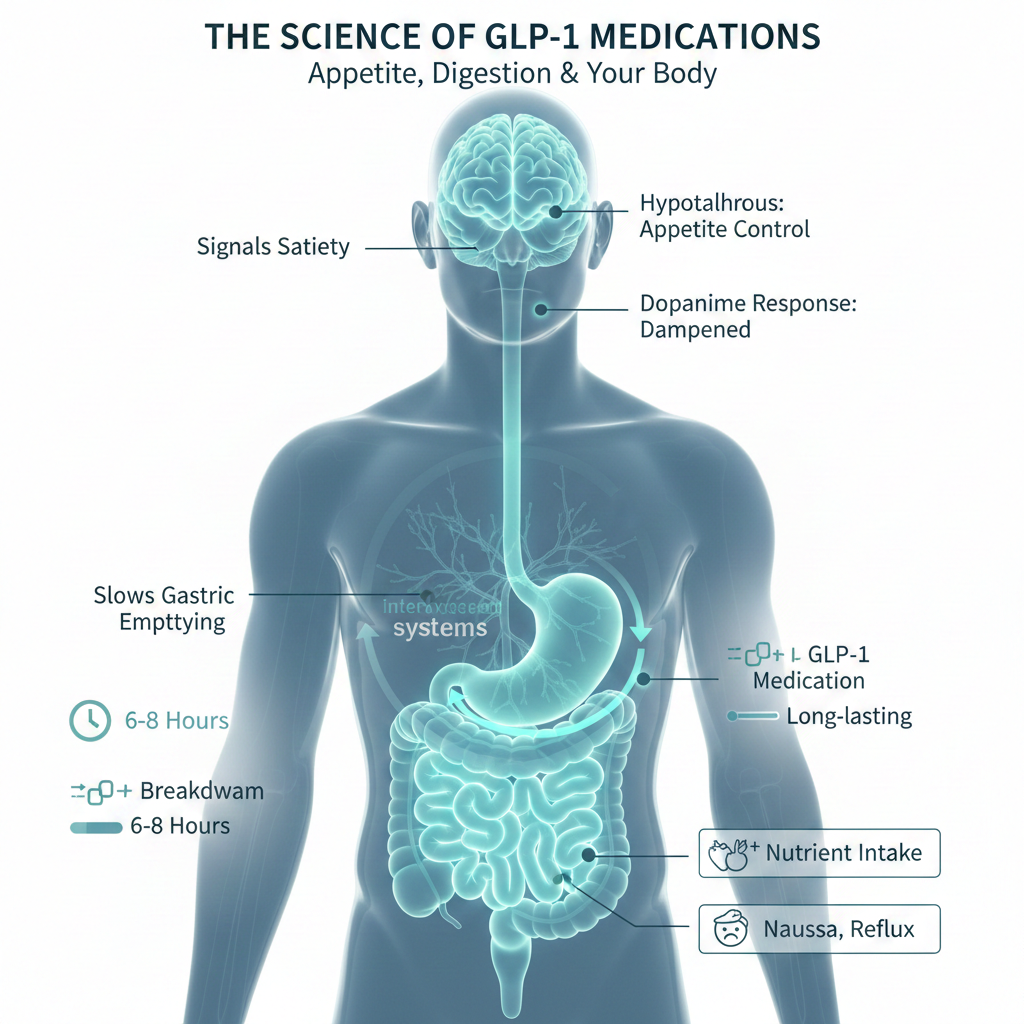
The brain effects prove particularly profound. GLP-1 receptors concentrate in the hypothalamus, the appetite control center, and in reward pathways that govern food pleasure. These medications activate satiety signals while simultaneously dampening the dopamine response to eating. Food becomes less appealing on multiple levels. Hunger diminishes. Cravings quiet. The mental preoccupation with eating that characterized previous weight struggles simply fades.
Simultaneously, gastric emptying slows dramatically. A typical meal that would clear the stomach in two to four hours may now take six to eight hours or longer. Food sits in the stomach far longer than the body evolved to expect, producing extended fullness but also the nausea, reflux, and discomfort that rank among the most common side effects.
These changes create both the opportunity and the challenge of GLP-1 therapy. Reduced appetite enables caloric restriction without constant hunger. But reduced intake also means reduced nutrient consumption unless food choices become extraordinarily intentional. Slower digestion creates prolonged satiety. But it also limits what the body can tolerate and process efficiently.
Every nutritional strategy for GLP-1 therapy flows from these physiological realities. For a deeper exploration of these mechanisms and their practical implications, the complete breakdown of how GLP-1 drugs change appetite and digestion provides the foundation for everything that follows.
Protein requirements and muscle preservation
The number on the scale tells only half the story. What matters equally is what comprises the weight being lost. And without deliberate intervention, GLP-1 medications produce body composition outcomes that undermine long-term health.

Clinical data from the STEP 1 trial, which led to Wegovy’s FDA approval, documented that approximately 39% of total weight lost came from lean mass rather than adipose tissue. For someone losing 50 pounds, that potentially means 20 pounds of muscle, bone density, and connective tissue sacrificed alongside the fat. This ratio far exceeds what obesity medicine specialists consider acceptable.
The phenomenon has grown common enough to earn its own terminology. “Ozempic body” describes the deflated, loose-skinned appearance that develops when someone loses substantial weight without preserving underlying muscle structure. Beyond aesthetics, this muscle loss slows metabolism, reduces functional strength, increases fall risk in older adults, and makes long-term weight maintenance substantially harder.
Preventing this outcome requires protein intake far exceeding standard recommendations. General guidelines suggesting 0.8 grams per kilogram of body weight were established for sedentary individuals maintaining stable weight. They were never designed for people losing weight rapidly on pharmaceutical appetite suppressants.
Research on weight loss and body composition consistently demonstrates that higher protein intakes preserve more lean mass during caloric restriction. For GLP-1 users, this means targeting 1.2 to 1.6 grams of protein per kilogram of body weight daily, roughly double the standard recommendation. For a 180-pound person, this translates to 98 to 131 grams of protein daily.
| Category | Protein Target | Example (180 lb person) |
| Minimum threshold | 1.2 g/kg body weight | 98 grams daily |
| Active weight loss | 1.4-1.6 g/kg body weight | 115-131 grams daily |
| With resistance training | 1.6-2.0 g/kg body weight | 131-164 grams daily |
| Older adults (65+) | 1.2-1.5 g/kg body weight | 98-123 grams daily |
The practical challenge emerges immediately. Most GLP-1 users struggle to eat 1,200 calories daily, let alone hit protein targets of 100+ grams. When appetite has vanished and three bites produce fullness, consuming adequate protein requires strategic prioritization that treats protein as the non-negotiable foundation of every eating occasion.
This means starting each meal with protein before touching carbohydrates or fats. It means choosing protein-dense foods that pack maximum amino acids into minimal volume. Greek yogurt, eggs, cottage cheese, and lean poultry become dietary staples. Protein shakes and supplements bridge gaps when whole food consumption falls short.
Timing matters alongside quantity. Spreading protein consumption throughout the day optimizes muscle protein synthesis better than consuming large amounts in a single meal. Aim for 25 to 35 grams of protein at each eating occasion rather than attempting to hit daily targets in one sitting.
The complete guide to protein needs on Ozempic and Wegovy provides specific food sources, timing strategies, and supplementation approaches for meeting these elevated requirements.
Protein alone does not fully protect muscle mass. Mechanical loading through resistance exercise tells your body that muscles are needed, providing the stimulus for preservation that nutrition alone cannot supply. Two to three resistance training sessions weekly, targeting all major muscle groups, combined with adequate protein intake can shift body composition dramatically toward fat loss rather than indiscriminate weight loss.
The detailed strategies for preventing muscle loss on GLP-1 medications address both the nutritional and exercise components of this critical challenge.
Micronutrient deficiencies and supplementation strategies
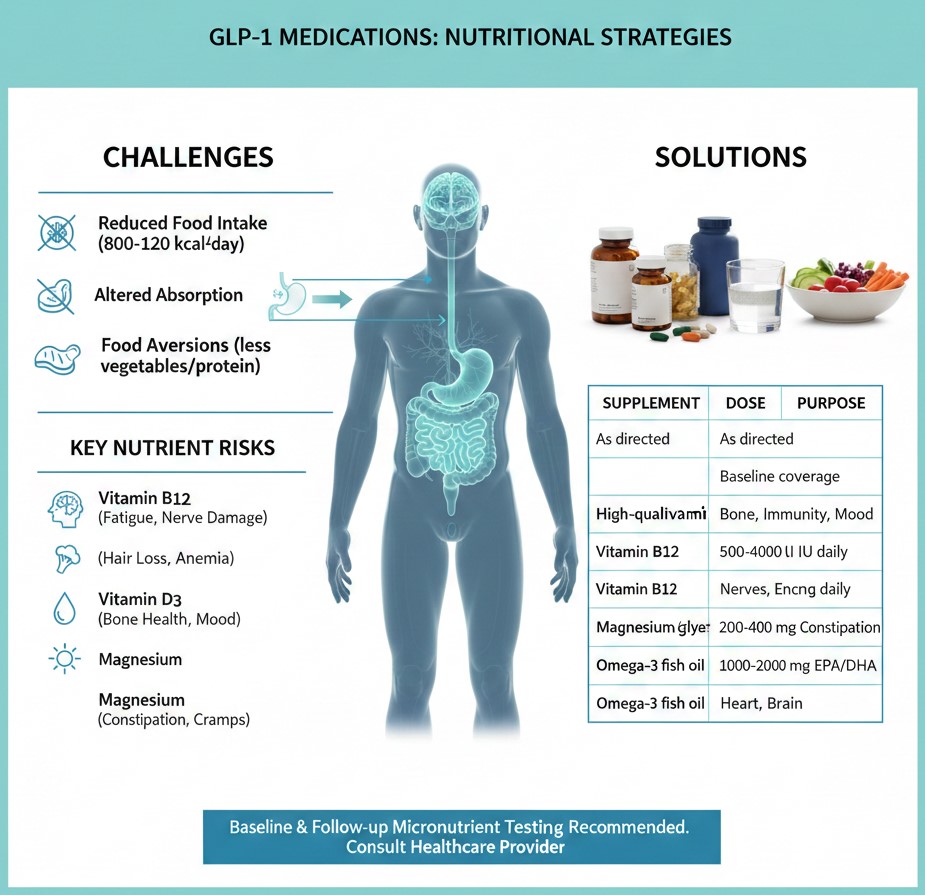
The mathematics of micronutrition change fundamentally when food intake drops by half. Standard dietary guidelines assume 1,800 to 2,200 calories daily for most adults. At this intake level, a reasonably varied diet typically provides adequate vitamins and minerals without supplementation. GLP-1 users frequently consume 800 to 1,200 calories daily. At these intake levels, meeting micronutrient needs through food alone becomes mathematically impossible regardless of food quality.

Beyond reduced intake, GLP-1 medications create additional absorption challenges. Delayed gastric emptying alters the timing and efficiency of nutrient uptake. Nausea and food aversions lead many users to avoid nutrient-dense foods like vegetables and proteins in favor of bland, easily tolerated options that offer fewer micronutrients per calorie. The gastrointestinal side effects common during dose titration further compound the problem through vomiting, diarrhea, and reduced appetite.
Several nutrients warrant particular attention during GLP-1 therapy.
Vitamin B12 deficiency has emerged as one of the most concerning nutritional consequences of treatment. These medications reduce gastric acid secretion and slow stomach emptying, both of which impair B12 absorption. Symptoms including fatigue, cognitive changes, numbness, and mood disturbances overlap significantly with commonly reported medication side effects, making deficiency easy to miss without blood testing. Long-term B12 deficiency causes irreversible neurological damage.
Iron deficiency affects a significant portion of the general population, particularly premenopausal women. Reduced food intake exacerbates existing insufficiency. The richest dietary iron sources, red meat and organ meats, are precisely the foods many GLP-1 users find difficult to tolerate. Hair loss, one of the most distressing complaints among users, frequently traces back to inadequate iron stores.
Vitamin D levels, already suboptimal in most Americans, drop further when fortified dairy products and fatty fish consumption decreases. This mineral supports bone health, immune function, muscle strength, and mood regulation. For individuals losing significant weight, maintaining vitamin D status becomes especially important as mechanical unloading from carrying less body weight already stresses bone density.
Magnesium deficiency affects an estimated 50% of the general American population before any dietary restriction. This mineral supports over 300 enzymatic reactions including muscle and nerve function, blood sugar regulation, and bone health. It also helps with constipation, one of the most common GLP-1 complaints.
The complete breakdown of vitamin deficiencies on weight loss drugs identifies which nutrients to monitor and the warning signs that suggest developing insufficiency.
Given these challenges, strategic supplementation shifts from optional to essential for most GLP-1 users. A reasonable baseline regimen includes:
| Supplement | Dose | Purpose |
| High-quality multivitamin | As directed | Baseline micronutrient coverage |
| Vitamin D3 | 2,000-4,000 IU daily | Bone health, immunity, mood |
| Vitamin B12 | 500-1,000 mcg daily | Neurological protection, energy |
| Magnesium glycinate or citrate | 200-400 mg daily | Muscle function, constipation relief |
| Omega-3 fish oil | 1,000-2,000 mg EPA/DHA | Cardiovascular and brain health |
Additional supplementation depends on individual circumstances. Protein powder becomes necessary when whole food protein intake falls short despite best efforts. Collagen peptides may support skin elasticity during rapid weight loss. Iron supplementation should only occur with documented deficiency confirmed through blood testing.
The evidence-based guide to supplements for GLP-1 users provides detailed recommendations for what to take, what to avoid, and how to work with healthcare providers on monitoring.
Baseline micronutrient testing before starting GLP-1 therapy provides valuable reference points. Follow-up testing at three to six month intervals during active weight loss helps catch developing deficiencies before symptoms become severe. Advocating for this testing as part of comprehensive GLP-1 management ensures deficiencies get caught early when correction is straightforward.
Digestive health, fiber, and hydration
The gastrointestinal system bears the most direct impact of GLP-1 therapy. Slowed motility throughout the digestive tract, combined with altered food intake patterns, creates challenges that require proactive management rather than reactive treatment.

Constipation affects approximately 24% of GLP-1 users, making it one of the most common persistent side effects. The mechanism is straightforward. Slower gastric emptying extends to slower transit through the entire intestinal tract. Reduced food volume means less bulk stimulating peristalsis. Lower fluid intake compounds the problem. The result ranges from mild discomfort to severe impaction that requires medical intervention.
Fiber intake provides the primary nutritional tool for managing digestive regularity. But fiber on GLP-1 therapy requires more nuance than simply eating more vegetables. When the stomach already empties slowly and fullness persists for hours, loading up on bulky high-fiber foods can worsen bloating, nausea, and the very discomfort you are trying to address.
The distinction between soluble and insoluble fiber matters here. Soluble fiber, found in oats, beans, apples, and psyllium, absorbs water and forms a gel that moves smoothly through the digestive tract. It feeds beneficial gut bacteria and generally offers gentler effects. Insoluble fiber, concentrated in wheat bran, raw vegetables, and whole grain skins, adds bulk but can create more gas and discomfort in a system already moving slowly.
Most GLP-1 users do better emphasizing soluble fiber sources while introducing insoluble fiber gradually. A reasonable target starts at 20 to 25 grams daily rather than the standard 25 to 35 gram recommendation, with increases based on tolerance.
| Fiber Source | Type | Serving | Fiber Content |
| Psyllium husk | Soluble | 1 tablespoon | 5 grams |
| Oatmeal | Primarily soluble | 1 cup cooked | 4 grams |
| Black beans | Mixed | 1/2 cup | 7.5 grams |
| Avocado | Primarily soluble | 1/2 medium | 5 grams |
| Raspberries | Mixed | 1 cup | 8 grams |
| Chia seeds | Primarily soluble | 2 tablespoons | 10 grams |
Fiber supplements offer a controlled approach when whole food fiber proves difficult to tolerate. Psyllium husk provides gentle, effective soluble fiber that rarely causes the bloating and gas associated with other supplements. Methylcellulose represents another well-tolerated option. Both should be introduced gradually and taken with generous water.
The comprehensive approach to fiber and gut health on GLP-1 therapy addresses the full spectrum of digestive challenges from constipation to bloating to maintaining a healthy microbiome during rapid dietary changes.
Hydration represents the often-overlooked partner to digestive health. GLP-1 medications suppress thirst signals alongside hunger signals. The same mechanisms that make you forget to eat make you forget to drink. Meanwhile, fluid needs may actually increase during rapid weight loss as the body processes metabolic waste from breaking down adipose tissue.
Signs of dehydration develop insidiously. Fatigue attributed to caloric restriction may actually reflect inadequate fluid intake. Headaches blamed on dose adjustment could trace to dehydration. Constipation worsens substantially when fluid intake drops.
Baseline fluid targets for GLP-1 users run higher than general recommendations. Aim for 80 to 100 ounces of total fluid daily, including water, tea, coffee, and water-rich foods. This requires active attention rather than relying on thirst cues that no longer function reliably.
Electrolyte balance shifts during GLP-1 therapy as well. Reduced food intake means reduced dietary sodium, potassium, and magnesium. Gastrointestinal side effects including vomiting and diarrhea can deplete electrolytes acutely. Muscle cramps, fatigue, heart palpitations, and dizziness may signal electrolyte imbalance rather than simple calorie restriction.
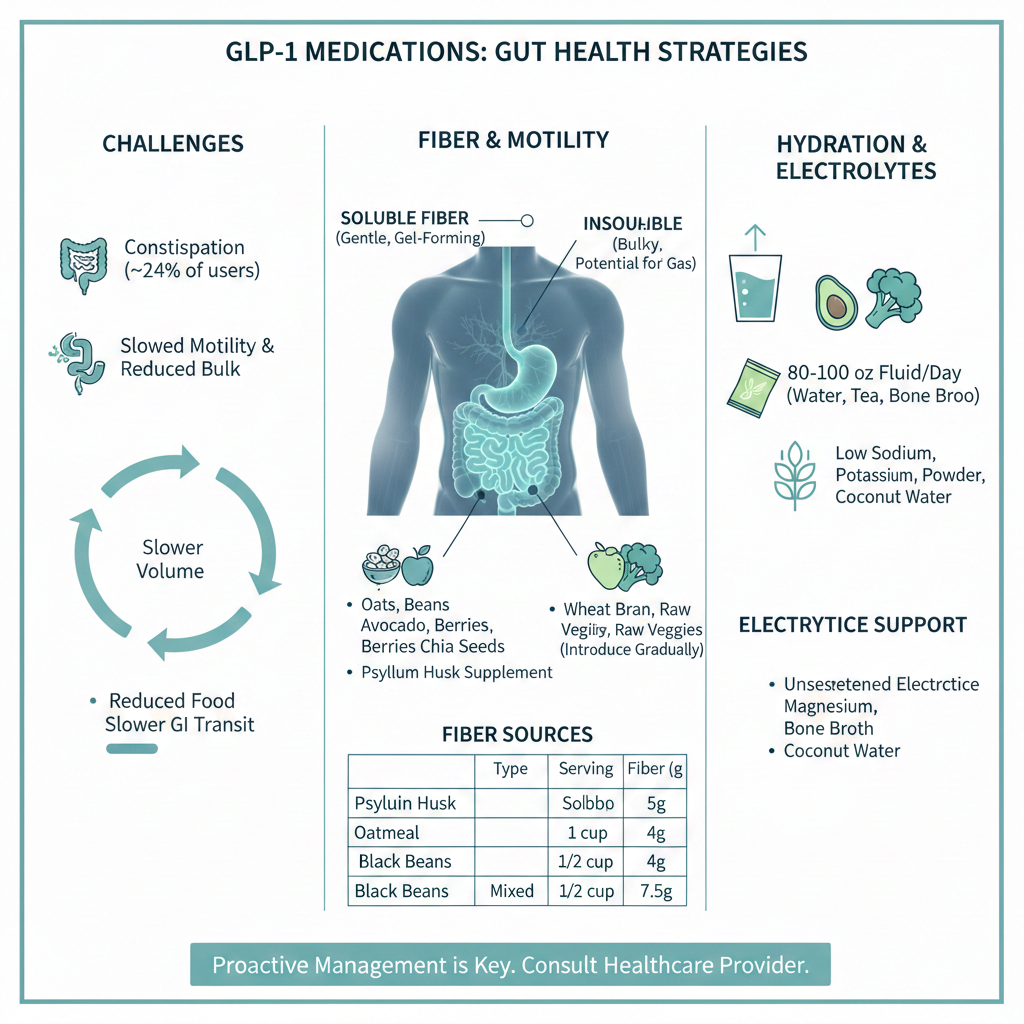
Strategic electrolyte management does not require sports drinks loaded with sugar. Unsweetened electrolyte powders, bone broth, coconut water, and deliberate inclusion of potassium-rich foods like avocado and leafy greens maintain balance without excessive calories.
The detailed guidance on hydration and electrolytes during GLP-1 therapy provides practical daily protocols for preventing the fluid and mineral imbalances that undermine energy and wellbeing.
Food choices, meal planning, and tolerability
When every bite counts and stomach capacity has shrunk dramatically, food selection shifts from general healthy eating principles to precise strategic choices. The foods that served weight loss efforts before GLP-1 therapy may not work now. The meals that once seemed moderate may become overwhelming. Success requires learning an entirely new relationship with food portions, timing, and composition.

Tolerance patterns change substantially on GLP-1 medications. Foods that presented no problems before treatment may trigger nausea, cramping, or prolonged discomfort. These changes stem directly from the altered digestive physiology rather than from psychological factors or food sensitivities.
High-fat foods consistently rank among the most problematic. Fat naturally slows gastric emptying. Combined with medication-induced delayed emptying, fatty meals can sit in the stomach for many hours, causing persistent fullness, nausea, and reflux. Fried foods, fatty cuts of meat, rich sauces, and creamy preparations often become intolerable regardless of how much they were enjoyed previously.
Greasy and heavily processed foods amplify these effects. Fast food, which typically combines high fat with large portions and rapid eating, creates a perfect storm of digestive distress. The convenience that made such foods appealing becomes outweighed by hours of subsequent discomfort.
Spicy foods trigger reflux and nausea for many users, particularly during dose escalation periods when the stomach is most sensitive. Carbonated beverages introduce gas into an already slow-moving system, worsening bloating and discomfort. Very sweet foods can cause dumping syndrome symptoms in some individuals, including cramping, sweating, and diarrhea.
Conversely, certain foods tend to be well tolerated across most GLP-1 users. These share common characteristics: moderate fat content, easy digestibility, and relatively bland flavor profiles.
| Well-Tolerated Foods | Why They Work |
| Eggs (poached, scrambled) | High protein, easy to digest, mild flavor |
| Greek yogurt | Protein-dense, smooth texture, probiotics |
| Poached or baked chicken | Lean protein, gentle on stomach |
| White fish | Low fat, easily digestible protein |
| Oatmeal | Soluble fiber, smooth texture, filling |
| Bananas | Gentle on stomach, natural electrolytes |
| Steamed vegetables | Nutrient-dense, softer texture |
| Cottage cheese | High protein, easy portions, mild |
The complete guide to best and worst foods on GLP-1 medications provides extensive lists of foods to emphasize and foods to limit based on common tolerance patterns and nutritional value.
Individual variation means your experience may differ from general patterns. Keeping a simple food and symptom log during the first months of treatment helps identify personal tolerability patterns. Note what you ate, how much, when, and how you felt in the following hours. Patterns emerge that guide increasingly personalized food choices.
Meal planning on GLP-1 therapy requires embracing structure that may feel unfamiliar. With appetite signals unreliable and eating capacity limited, planned eating occasions replace intuitive eating. This is not permanent. It is a strategic adaptation to temporary physiological circumstances.
Two approaches work for different users. Some do better with two larger meals daily, allowing adequate time for complete digestion between eating occasions. Others prefer three smaller meals plus one protein-rich snack. Neither pattern is inherently superior. The right choice depends on your schedule, tolerance patterns, and ability to meet protein targets within each framework.
Timing around medication doses matters for some users. Nausea often peaks in the 24 to 48 hours following injection. Planning lighter, easier-to-tolerate meals during this window and saving more ambitious eating for days when symptoms recede helps manage intake across the week.
The detailed approach to meal planning on GLP-1 therapy offers sample meal frameworks, timing strategies, and approaches for managing difficult days when eating anything feels challenging.
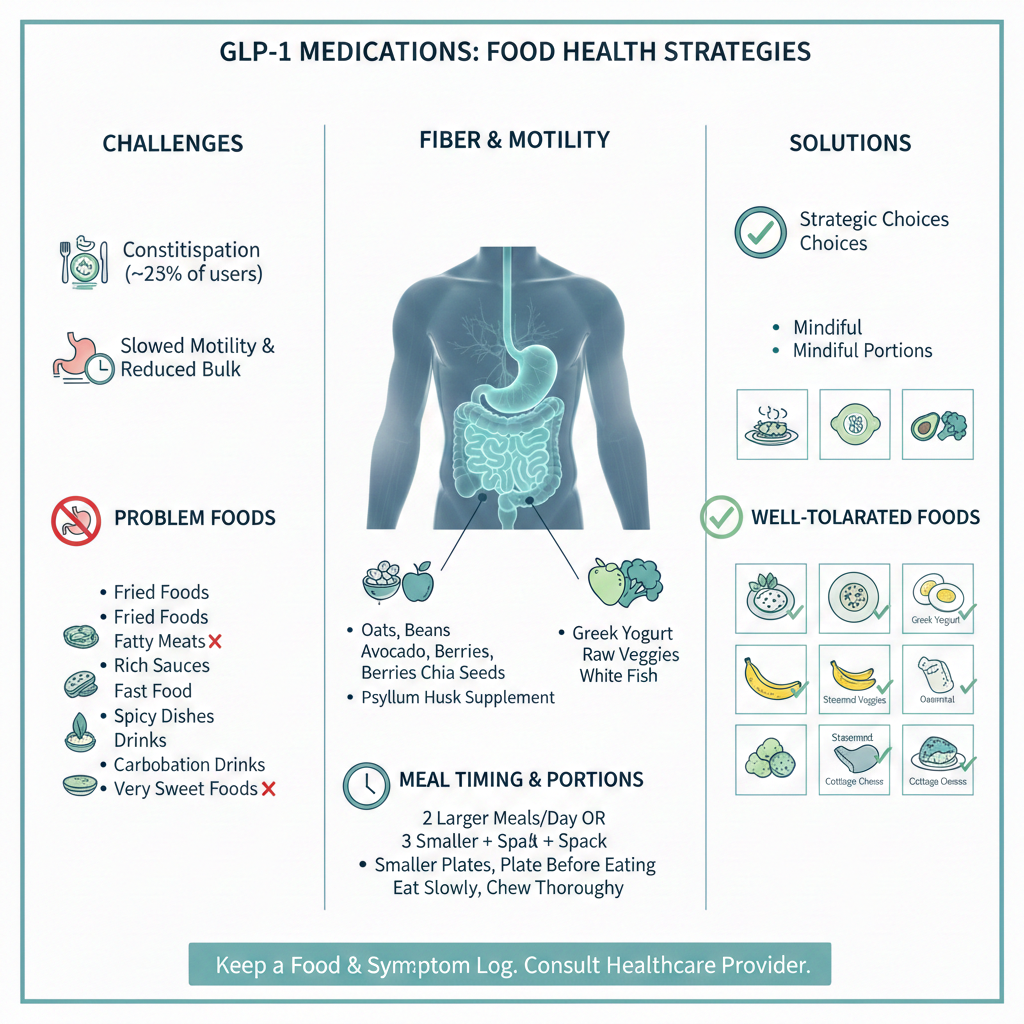
Portion sizes require complete recalibration. What looks like an appetizer now constitutes a meal. The portion that previously seemed reasonable may now represent two or three eating occasions worth of food. Visual estimation fails because reference points no longer apply.
Practical portion guidance includes using smaller plates to make appropriate portions look adequate, plating food before sitting down rather than serving family style, and accepting that half a restaurant entree may be the right amount even when it looks absurdly small. Ordering appetizers as entrees or sharing plates becomes practical rather than stingy.
Eating pace slows dramatically from necessity. Rushing leads to overconsumption before fullness signals arrive, followed by hours of regret. Taking small bites, chewing thoroughly, pausing between bites, and putting down utensils periodically helps pace intake appropriately.
Life after treatment and long-term maintenance
The medication was never meant to be permanent for everyone. Insurance coverage lapses. Treatment goals are reached. Side effects become intolerable. Supply shortages make continuation impossible. Whatever the reason, the question that haunts most GLP-1 users eventually demands an answer: what happens when this stops?

The statistics offer sobering context. Research published in the New England Journal of Medicine documented that patients regain approximately two-thirds of lost weight within one year of discontinuing semaglutide. Some regain everything and more. A fortunate minority maintains their results. The difference between these outcomes traces almost entirely to what happened during treatment rather than what happens after it ends.
This reality reframes the entire purpose of GLP-1 therapy. The medication does not fix obesity. It provides a window of reduced appetite during which the actual work of building sustainable habits either happens or does not happen. Those who use the window to develop new skills, preferences, and behaviors have a foundation for maintenance. Those who simply enjoy effortless restriction without behavioral investment find themselves unprepared when the pharmaceutical scaffolding disappears.
Weight regain after discontinuation occurs through multiple mechanisms that operate simultaneously.
Appetite returns, often intensely. The hypothalamic and reward pathway effects that suppressed hunger reverse when medication clears the system. Many users report appetite returning stronger than before treatment, a phenomenon sometimes called rebound hunger. The quiet mind that no longer obsessed about food becomes loud again.
Metabolic adaptations persist. Rapid weight loss triggers defensive responses designed to protect against starvation. Resting metabolic rate decreases. Hunger hormones increase. The body becomes more efficient at extracting and storing calories. These adaptations do not immediately resolve when medication stops. The body remains primed for regain.
Muscle loss during treatment compounds the challenge. Users who lost significant lean mass face reduced daily calorie expenditure. The caloric intake that maintains their new weight has decreased, making the margin for error smaller than it was at the same weight before treatment.
The comprehensive guide to weight maintenance after stopping GLP-1 therapy addresses specific strategies for navigating this challenging transition.
Preparation for eventual discontinuation should begin immediately, not when treatment ends. Every day of GLP-1 therapy represents an opportunity to practice the skills needed when medication is gone.
This means treating reduced appetite as a training opportunity rather than a free pass. The medication makes eating less dramatically easier. Use that ease to build genuine habits rather than simply enjoying effortless restriction. Pay attention to portions even when you naturally eat less. Develop hunger recognition skills even when signals are blunted. Build sustainable food preferences that will persist without pharmaceutical assistance.
Exercise habits established during treatment transfer more reliably than dietary changes. Physical activity that becomes routine during treatment requires less willpower to maintain afterward. Resistance training that preserves muscle during weight loss continues supporting metabolic rate and body composition during maintenance.
Emotional eating patterns addressed during treatment stay addressed. For many people, excess weight developed partly through emotional relationships with food. GLP-1 medications temporarily break these patterns by suppressing food reward. Without deliberate work on underlying triggers, these patterns reassert themselves when medication stops.
The first three to six months after discontinuation represent the highest risk period for regain. Appetite returns, often aggressively. Old habits reassert themselves. The scale begins moving in the wrong direction. Deliberate strategies for this transition period improve outcomes substantially.
Increased monitoring during transition helps catch problems early. Weighing daily or every other day provides early warning when a five-pound regain allows intervention before it becomes fifty pounds. Tightening dietary structure during the transition period, with meal planning, food logging, and deliberate eating, provides guardrails when internal appetite regulation cannot be trusted.
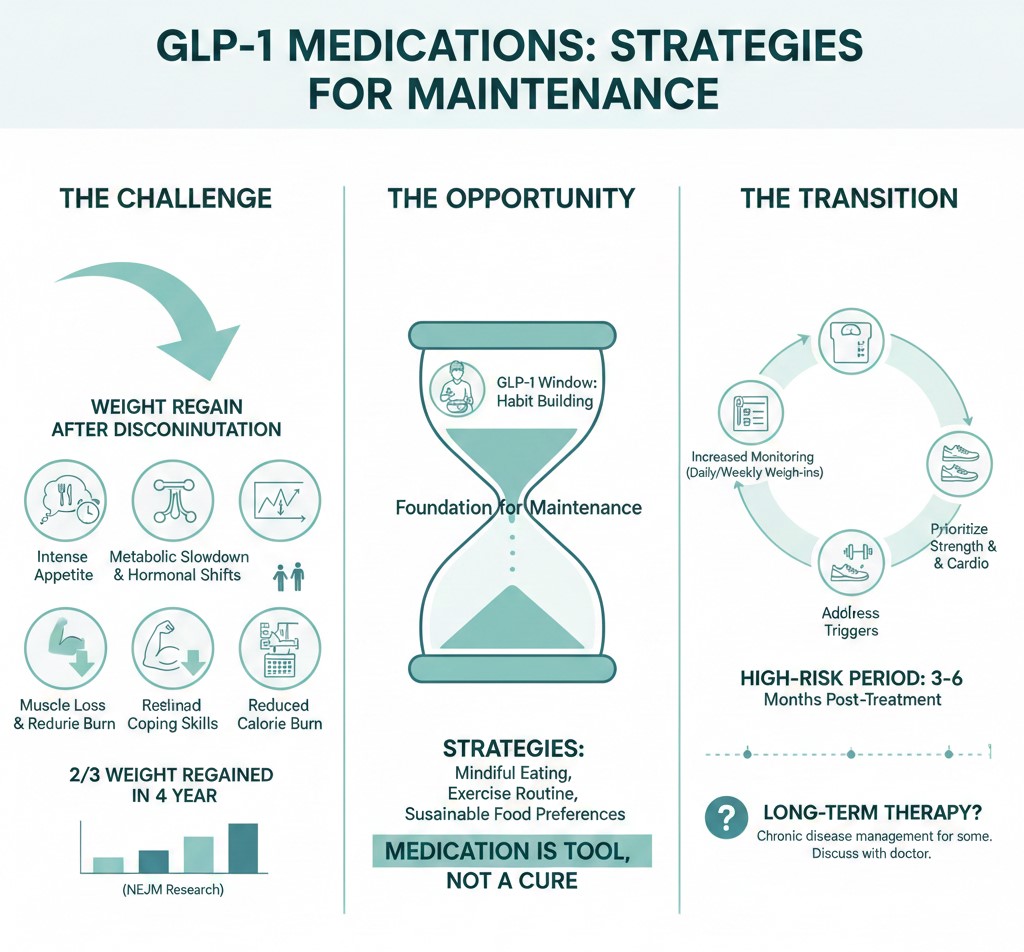
Some individuals cannot maintain weight loss without medication despite best efforts. This is not personal failure. It reflects the biological reality that obesity involves hormonal and neurological factors not fully overcome by behavior change alone. Long-term or indefinite GLP-1 use may be appropriate for some patients. These medications are increasingly viewed as chronic disease management rather than temporary intervention.
The goal remains sustainable health rather than a particular number on the scale. Maintaining a weight somewhat above your lowest medication-assisted weight but below your starting weight still provides meaningful health benefits. Perfect should not be the enemy of good.
Navigating the new normal
The transformation GLP-1 medications produce extends far beyond the scale. Appetite functions differently. Digestion operates on an altered timeline. The relationship between food and pleasure has shifted. Nutritional needs have intensified even as eating capacity has diminished. These changes demand not just different food choices but an entirely reconstructed approach to nourishment.
The medical system that readily prescribes these medications rarely provides adequate nutritional guidance for navigating them. A brief instruction to eat less and move more misses the profound physiological shifts that make standard weight loss advice insufficient. The responsibility for learning how to eat well during treatment falls largely on patients themselves.
What emerges from this challenge, when approached deliberately, is a more intentional and informed relationship with food than most people have ever developed. The constraints of GLP-1 therapy force attention to questions that unrestricted eating never demanded. Which foods truly nourish? What does the body actually need versus what appetite historically demanded? How can maximum nutrition be delivered in minimum volume? What habits will persist when pharmaceutical assistance ends?
These questions matter beyond GLP-1 therapy. The answers developed through this period of constrained eating create foundations applicable for life. Understanding protein requirements, recognizing hydration needs, appreciating the role of specific micronutrients, and building meal structures that support goals rather than undermine them constitute nutritional literacy that serves long after treatment ends.
The medication opened a door. What gets built on the other side depends entirely on the intentionality brought to treatment. Those who use this window to develop genuine skills, preferences, and habits find themselves better equipped for long-term health than they were before treatment began. Those who simply wait for the drug to do the work arrive at a lower weight without the tools to stay there.
Every section of this GLP-1 nutrition guide addresses a specific challenge within the larger project of eating well during treatment. Protein preservation protects the body composition that supports lasting results. Micronutrient attention prevents the deficiencies that undermine energy and wellbeing. Digestive strategies manage the side effects that make treatment tolerable. Food selection and meal planning translate understanding into daily practice. Maintenance preparation ensures the work done during treatment persists beyond it.

The starting point for most users should be protein. Without adequate protein intake and the muscle preservation it supports, weight loss produces outcomes that undermine long-term health regardless of how impressive the scale numbers appear. The detailed guidance on protein needs for Ozempic and Wegovy users provides the foundation upon which everything else builds.
GLP-1 medications represent a genuine breakthrough in obesity treatment. They make possible what willpower alone could not achieve for millions of people. But they remain tools rather than solutions. The solution lies in what gets done with the opportunity they create.
What will you build with yours?
1 Comment
-
This was such a helpful read! I really liked how clear and practical it was, without making things feel too complicated. It’s reassuring to see nutrition explained in a way that feels realistic and actually useful for people on GLP-1 medications.