




The first bite told her something had fundamentally shifted. Not just reduced hunger, which she expected. The entire experience of eating had transformed. Food that once triggered pleasure now registered as merely functional. The urgent drive to finish everything on the plate had vanished. And somewhere around bite three, a signal arrived that had been absent for decades: enough.
This is not willpower. It is not discipline finally kicking in after years of failed diets. It is pharmacology, a precise intervention in the hormonal and neurological systems that govern appetite, satiety, and digestive function. Understanding exactly what GLP-1 medications do to these systems explains why eating changes so dramatically, why certain side effects occur, and why specific nutritional strategies work while others fail.
The more you understand the mechanism, the better you can work with it rather than against it.
GLP-1 receptor agonists are a class of injectable medications originally developed to treat type 2 diabetes. They mimic glucagon-like peptide-1, a natural hormone that regulates blood sugar, slows gastric emptying, and signals fullness to the brain.
Because they significantly reduce appetite, several GLP-1 medications are now FDA-approved for chronic weight management in adults with obesity or overweight with related health conditions.
Common examples: Ozempic and Wegovy (semaglutide), Mounjaro and Zepbound (tirzepatide), Saxenda (liraglutide), and Trulicity (dulaglutide).
What GLP-1 actually is
GLP-1 stands for glucagon-like peptide-1, a hormone your body produces naturally in the intestines after eating. Under normal circumstances, GLP-1 performs several functions: it stimulates insulin release, suppresses glucagon secretion, slows gastric emptying, and signals satiety to the brain.
The problem is that natural GLP-1 breaks down within minutes. Its effects are fleeting, providing only brief post-meal satiety before hunger returns.
Medications like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) are modified versions of GLP-1 that resist breakdown. A single weekly injection maintains elevated GLP-1 activity for days rather than minutes. The effects that normally last briefly after meals become continuous.
This sustained GLP-1 activity produces the dramatic appetite suppression and weight loss these medications have become famous for. But it also creates the digestive changes and side effects that shape daily eating experiences.
The brain effects: rewiring appetite and reward
GLP-1 receptors exist throughout the body, but some of the most consequential are located in the brain. These receptors concentrate in areas governing appetite regulation and reward processing.
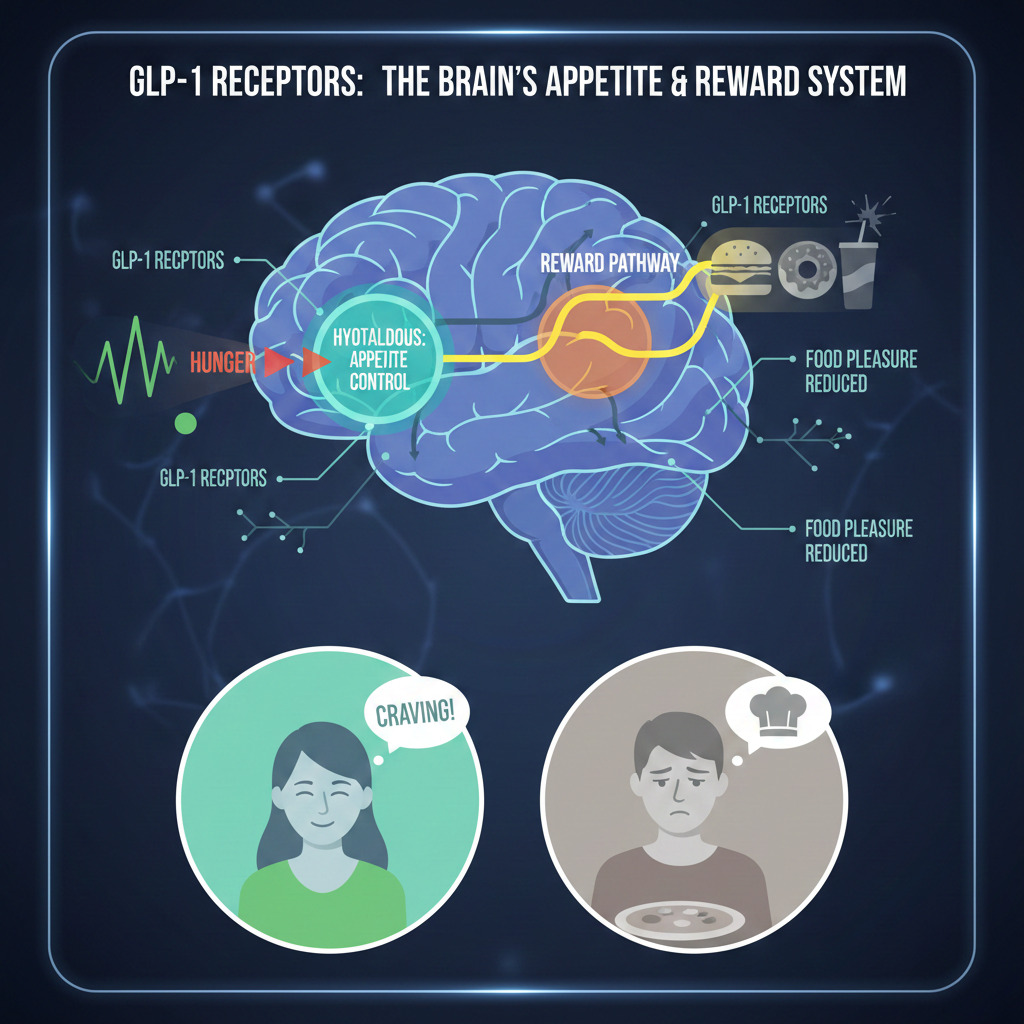
Hypothalamic effects: The hypothalamus serves as the brain’s appetite control center, integrating signals about energy status and directing eating behavior. GLP-1 medications activate receptors here that suppress hunger signals and enhance satiety. The result is reduced baseline appetite, diminished food-seeking behavior, and earlier fullness during meals.
Reward pathway modulation: Perhaps more profoundly, GLP-1 medications affect the brain’s reward system. Food normally triggers dopamine release that creates pleasure and reinforces eating behavior. These medications dampen this reward response, reducing the pleasure derived from eating.
This explains why food often loses its appeal beyond mere hunger reduction. Favorite foods may no longer seem worth the effort. The anticipation and enjoyment that once surrounded meals diminishes. Some users describe food becoming almost boring, a necessary task rather than a source of pleasure.
For those whose weight struggles involved food addiction or emotional eating patterns, this reward reduction can feel liberating. The constant mental preoccupation with food quiets. Cravings lose their power. The voice demanding another serving finally goes silent.
For others, particularly those who genuinely enjoyed food as a positive life experience, the diminished pleasure creates a sense of loss. Food-centered social occasions lose appeal. Cooking no longer brings joy. This psychological shift requires adjustment even as the scale moves in the desired direction.
Gastric emptying: the slowdown effect
One of GLP-1’s most significant peripheral effects occurs in the stomach. These medications dramatically slow gastric emptying, the rate at which food moves from the stomach into the small intestine.
Under normal conditions, a typical meal empties from the stomach in two to four hours. On GLP-1 therapy, this may extend to six to eight hours or longer. Food sits in the stomach substantially longer than the body evolved to expect.
This prolonged gastric residence produces several consequences:
Extended fullness: With food remaining in the stomach longer, the physical sensation of fullness persists well beyond normal duration. A moderate lunch may leave you feeling full through dinner. This extended satiety directly supports reduced calorie intake.
Nausea and discomfort: When the stomach expects to empty at its normal rate but cannot, nausea often results. This is why nausea ranks among the most common GLP-1 side effects, particularly during dose escalation when the body has not adapted.
Altered meal tolerance: Foods that digest slowly, particularly high-fat meals, compound the delayed emptying effect. What once seemed like a reasonable portion becomes overwhelming when the stomach cannot process it at normal speed.
Reflux risk: A fuller stomach for longer periods increases pressure that can push contents upward. Heartburn and acid reflux occur more frequently, especially when lying down after eating.
Intestinal and metabolic effects
Beyond the stomach, GLP-1 medications influence the entire gastrointestinal tract and metabolic function.
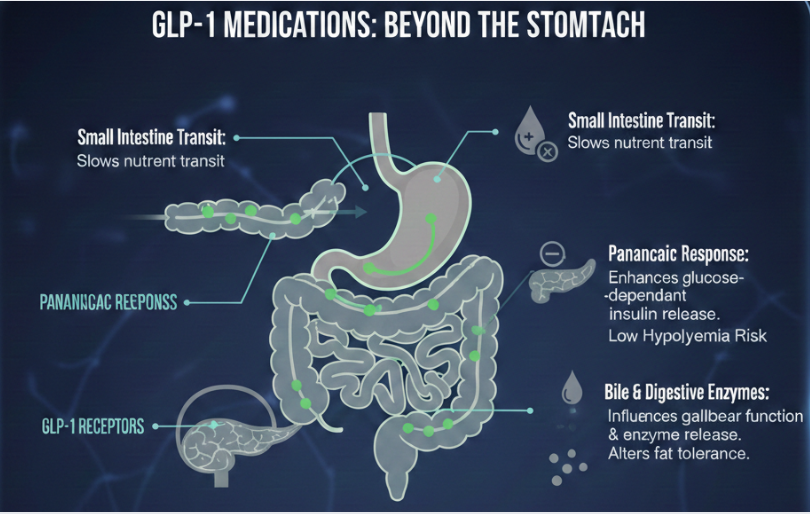
Small intestine transit: The slowing effect extends beyond the stomach. Food moves through the small intestine more slowly, potentially affecting nutrient absorption timing and efficiency.
Pancreatic response: GLP-1 enhances glucose-dependent insulin secretion. When blood sugar rises after eating, insulin release is amplified. When blood sugar is normal, the effect is minimal, reducing hypoglycemia risk compared to some diabetes medications.
Glucagon suppression: GLP-1 reduces glucagon secretion, the hormone that raises blood sugar. This contributes to improved glycemic control in diabetic patients and may help stabilize blood sugar in non-diabetic users.
Bile and digestive enzyme secretion: Some evidence suggests GLP-1 affects gallbladder function and digestive enzyme release. This may contribute to the altered fat tolerance many users report.
The side effect spectrum
Understanding the mechanism explains why specific side effects occur and suggests strategies for management.
Nausea
The most common side effect stems directly from slowed gastric emptying. The stomach signals distress when it cannot process contents at expected rates. Nausea typically peaks during dose escalation and often improves as the body adapts over weeks to months.
Management strategies include eating smaller portions, avoiding high-fat foods, eating slowly, and not lying down immediately after meals. For some users, nausea remains problematic throughout treatment, requiring dose adjustment or discontinuation.
Constipation
Slowed motility throughout the GI tract, combined with reduced food volume and often inadequate fiber and fluid intake, creates constipation for up to 24% of users. Our detailed article on fiber and GLP-1 therapy addresses this common challenge.
Diarrhea
Paradoxically, some users experience diarrhea rather than constipation. This may relate to fat malabsorption when the gallbladder does not empty properly, or to individual variations in how the gut responds to altered motility patterns.
Decreased Appetite for Specific Foods
Many users develop strong aversions to foods they previously enjoyed. Rich, fatty, sweet, or heavy foods commonly trigger disgust rather than desire. This is not purely psychological. It reflects altered reward processing and learned associations between certain foods and the nausea or discomfort they now cause.
Taste Changes
Some users report that foods taste different on GLP-1 medications. Sweetness may become cloying. Savory foods may lose appeal. Whether this reflects direct effects on taste receptors or secondary effects through reward pathway changes remains unclear.
How these changes affect nutritional needs
The physiological changes GLP-1 medications produce directly inform the nutritional strategies that work during treatment.
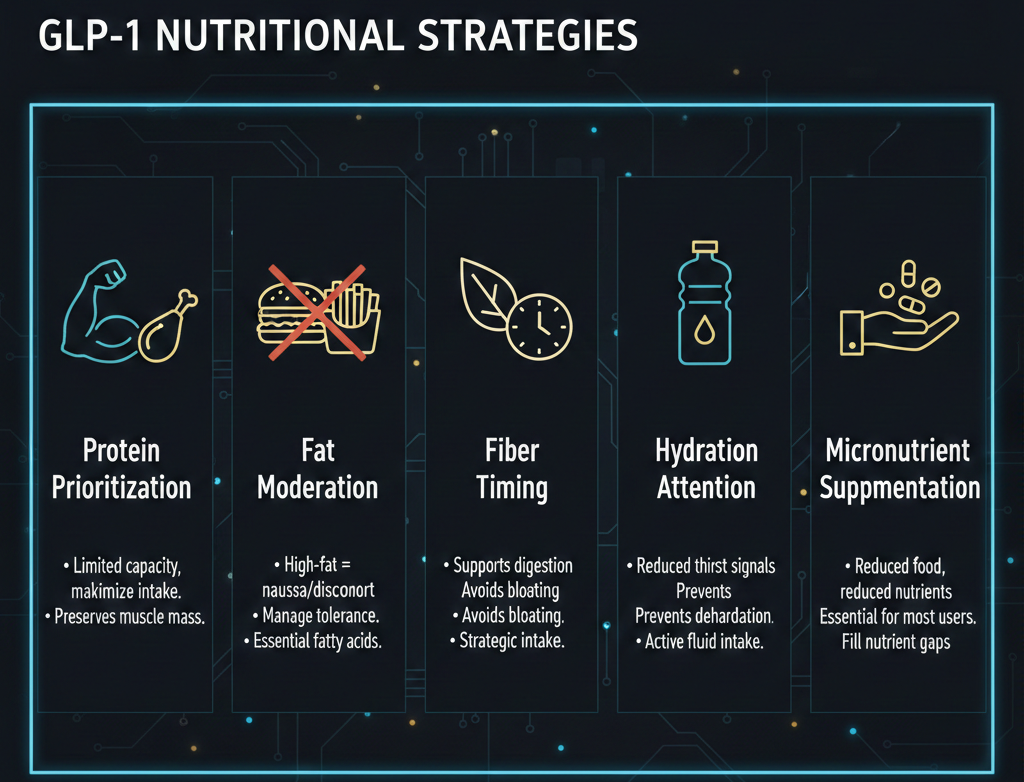
Protein prioritization: With limited eating capacity due to early fullness, every bite must count. Protein provides essential amino acids for muscle preservation in a situation where muscle loss represents a real risk. The strategies outlined in our article on protein needs for GLP-1 users address this requirement.
Fat moderation: High-fat foods exacerbate delayed gastric emptying and commonly trigger nausea and discomfort. Moderating fat intake while ensuring adequate essential fatty acid consumption helps manage tolerance. Our guidance on best and worst foods for GLP-1 users provides specific recommendations.
Fiber timing: Fiber supports digestive function but can worsen fullness and bloating when consumed in large amounts or at wrong times. Strategic fiber intake maintains gut health without overwhelming an already slowed system.
Hydration attention: Reduced thirst signals parallel reduced hunger signals. Active hydration strategies prevent the dehydration that commonly develops unnoticed. Our article on hydration and electrolytes during GLP-1 therapy covers this essential topic.
Micronutrient supplementation: Reduced food intake means reduced nutrient intake. The mathematics of micronutrition change fundamentally, making supplementation important for most users as detailed in our supplements article.
Individual variation in response
Not everyone responds identically to GLP-1 medications. Genetic variations in GLP-1 receptors, differences in baseline gut motility, varying reward system sensitivity, and numerous other factors create a spectrum of experiences.
Some users experience profound appetite suppression from low doses. Others require maximum doses for meaningful effect. Side effects that devastate one person barely register for another. Food tolerances vary unpredictably.
This variation explains why general guidelines require individual adjustment. What works for someone else may not work for you. Personal experimentation, guided by understanding of the underlying mechanisms, helps identify your optimal approach.
Working with your changed physiology
The transformation GLP-1 medications produce is not something to fight against. It is something to work with strategically.
Your appetite has changed. Honor that by eating when genuinely hungry rather than by schedule. Your stomach processes food differently. Respect that by choosing foods and portions it can handle. Your reward system responds differently to food. Accept that eating may become more functional and less recreational.
These changes enable weight loss that seemed impossible before. They also require nutritional strategies adapted to new physiological realities. The comprehensive approach outlined in our complete guide to GLP-1 nutrition addresses each element, from protein to fiber to hydration to supplements, within the context of how these medications alter normal function.
Understanding what is happening inside your body transforms the GLP-1 experience from confusing and sometimes frustrating to navigable and empowering. The medication changes the playing field. Knowledge helps you succeed on that new terrain.
What aspect of how GLP-1 medications affect your body has surprised you most since starting treatment?