





The injection that changed everything eventually stops. Maybe insurance coverage ends. Perhaps you reach your goal weight and decide to discontinue. Or side effects become intolerable and continuing no longer makes sense. Whatever the reason, the question that haunted you from day one finally demands an answer: what happens now?
The statistics are not encouraging. Studies show that patients regain approximately two-thirds of lost weight within one year of stopping GLP-1 medications. Some regain everything. A few maintain their results. The difference between these outcomes lies almost entirely in what happens during treatment, not after it ends.
The medication was never going to be the permanent solution. It was always a tool, a window of reduced appetite that either gets used to build sustainable habits or gets wasted waiting for the drug to do work that only behavior change can accomplish.
Why weight regain happens after GLP-1 discontinuation?
Understanding the mechanisms behind post-medication weight regain helps explain why maintenance requires deliberate strategy rather than hope.
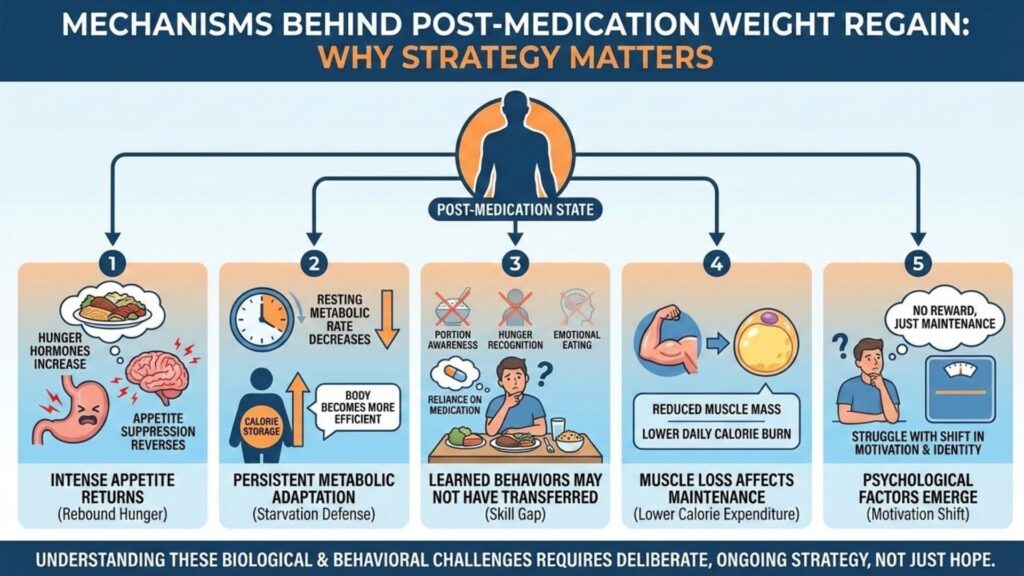
Appetite returns, often intensely: GLP-1 medications suppress appetite through multiple pathways, slowing gastric emptying, reducing hunger hormones, and affecting reward centers in the brain. When the medication clears your system, these effects reverse. Many users report appetite returning stronger than before treatment, a phenomenon sometimes called rebound hunger.
Metabolic adaptation persists: Rapid weight loss triggers metabolic adaptations designed to defend against starvation. Resting metabolic rate decreases. Hunger hormones increase. The body becomes more efficient at extracting and storing calories. These adaptations do not immediately resolve when medication stops. Your body remains primed for weight regain.
Learned behaviors may not have transferred: If you relied primarily on medication-induced appetite suppression to eat less, you may not have developed the skills needed to manage eating without that chemical assistance. Portion awareness, hunger recognition, emotional eating management, and food environment control all require practice that medication can mask.
Muscle loss affects maintenance capacity: Users who lost significant muscle alongside fat face a double challenge. Reduced muscle mass means lower daily calorie expenditure. The caloric intake that maintains weight has decreased, making the margin for error smaller.
Psychological factors emerge: The transition from losing weight to maintaining weight involves a significant psychological shift. Losing provides constant positive feedback as the scale drops. Maintenance offers no such reward, just the absence of negative change. Many people struggle with this shift in motivation and identity.
The maintenance mindset starts during treatment

The most important insight about post-GLP-1 maintenance is that it begins now, not later. Every month of treatment is an opportunity to practice the skills you will need when the medication is gone.
This means treating reduced appetite as a training opportunity rather than a free pass. Yes, the medication makes eating less dramatically easier. Use that ease to build habits rather than simply enjoying effortless restriction.
Practice portion awareness: Even though you naturally eat less on medication, pay attention to portions. Learn what appropriate serving sizes look like. Understand how much food your body actually needs versus how much you historically consumed. This knowledge transfers when appetite returns.
Develop hunger recognition: GLP-1 medications blur hunger signals, making it difficult to distinguish physical hunger from habit, boredom, or emotion. Practice checking in with yourself before eating. Ask whether you are genuinely hungry or eating for other reasons. This skill becomes crucial when appetite regulation returns to your responsibility.
Build sustainable food preferences: The dietary patterns you establish during treatment become your baseline for maintenance. If you rely on protein shakes and avoid learning to cook nutritious meals, you lack tools for the long term. Use treatment time to develop genuine enjoyment of nutrient-dense foods.
Establish exercise habits: Physical activity during treatment serves multiple purposes. It preserves muscle mass, supports metabolic health, improves mood, and creates habits that continue post-medication. Exercise that becomes routine during treatment requires less willpower to maintain afterward.
Address emotional eating patterns: For many people, excess weight developed partly through emotional relationships with food. GLP-1 medications suppress the reward response to food, temporarily breaking these patterns. Without deliberate work on underlying emotional eating triggers, these patterns return when medication stops.
Nutritional strategies for sustainable maintenance
The nutritional principles that support GLP-1 therapy also support long-term maintenance, though implementation shifts when appetite returns.
Protein remains paramount
High protein intake supports maintenance through multiple mechanisms. Protein provides greater satiety than carbohydrates or fat, helping control appetite naturally. It preserves muscle mass, maintaining metabolic rate. It requires more energy to digest, slightly increasing calorie expenditure.
Maintenance protein targets remain similar to treatment targets: 1.2 to 1.6 grams per kilogram of body weight daily. The difference is that achieving these targets becomes harder without medication-suppressed appetite making you naturally eat less of everything including protein.
Planning protein at every meal, starting meals with protein, and including protein-rich snacks helps maintain adequate intake when unrestricted appetite might otherwise lead toward carbohydrate-heavy choices.
Fiber supports satiety
Fiber provides bulk and satiety that partially compensates for the loss of medication-induced fullness. High-fiber foods slow digestion, moderate blood sugar response, and feed beneficial gut bacteria.
Maintaining fiber intake of 25 to 30 grams daily through vegetables, fruits, legumes, and whole grains supports appetite management. The fiber strategies developed during treatment, covered in our article on fiber and GLP-1 therapy, remain valuable for maintenance.
Caloric awareness without obsession
Maintenance requires eating at your new, lower caloric needs rather than your pre-treatment intake. This sounds obvious but proves challenging in practice.
A person who previously maintained 200 pounds eating 2,500 calories daily cannot return to that intake at 150 pounds without regaining weight. Their new maintenance calories might be 1,800 to 2,000. The 500 to 700 calorie daily difference adds up quickly.
Periodic calorie tracking, even if not daily, helps maintain awareness of intake. Knowing approximately what you consume prevents the gradual creep that leads to regain.
Meal structure and timing
Regular meal timing helps regulate appetite and prevents the excessive hunger that leads to overeating. Skipping meals often backfires through later overconsumption.
The meal patterns established during treatment, whether two larger meals or three smaller ones, can continue during maintenance. Consistency in timing helps the body establish predictable hunger patterns.
The critical role of physical activity
Exercise becomes even more important for maintenance than it was during active weight loss. Multiple mechanisms explain this relationship.
Metabolic rate support: Regular exercise, particularly resistance training, helps maintain or rebuild muscle mass. This muscle supports metabolic rate, increasing daily calorie expenditure and providing more margin for dietary flexibility.
Appetite regulation: Paradoxically, regular exercise often improves appetite regulation rather than simply increasing hunger. Active individuals tend to show better alignment between hunger signals and actual caloric needs.
Psychological benefits: Exercise provides mood regulation, stress management, and sense of accomplishment that can otherwise get sought through food. Maintaining an exercise identity supports weight management identity.
Practical calorie buffer: Each hour of moderate exercise burns several hundred calories. Regular activity creates practical room for occasional dietary indulgences without weight gain.
Maintenance exercise recommendations include both cardiovascular activity for health and calorie expenditure, and resistance training for muscle preservation. A realistic target includes 150 to 300 minutes of moderate cardio weekly plus two to three resistance training sessions.
Managing the transition period
The first three to six months after stopping GLP-1 medication represent the highest risk period for regain. Appetite returns, sometimes aggressively. Old habits reassert themselves. The scale begins moving in the wrong direction.
Deliberate strategies for this transition period improve outcomes.
Consider gradual discontinuation: If medically appropriate, tapering medication rather than stopping abruptly may ease the appetite transition. Discuss this option with your prescribing physician.
Increase monitoring: Weigh yourself regularly during the transition, perhaps daily or every other day. Catching a five-pound regain allows intervention before it becomes a fifty-pound regain. The scale provides early warning.
Tighten dietary structure: The transition period is not the time for flexible, intuitive eating. Meal planning, food logging, and structured eating provide guardrails when internal appetite regulation cannot be trusted.
Lean on support systems: Whether through professional support, weight loss communities, or personal relationships, social accountability helps maintain commitment during difficult transitions.
Have a plan for slip-ups: Occasional overeating will happen. The difference between a temporary slip and full relapse lies in response. A single high-calorie day means returning to normal eating the next day, not abandoning efforts entirely.
When maintenance is not working
Despite best efforts, some individuals cannot maintain weight loss without medication. This is not personal failure. It reflects the biological reality that obesity involves hormonal and neurological factors not fully overcome by behavior change alone.
Options for those struggling with maintenance include:
Returning to GLP-1 therapy: Long-term or indefinite GLP-1 use may be appropriate for some patients. These medications are increasingly viewed as chronic disease management rather than temporary intervention.
Trying alternative medications: Other weight management medications with different mechanisms may support maintenance for some individuals.
Intensive behavioral programs: Structured programs with regular professional contact provide accountability and support that self-management cannot match.
Accepting a higher stable weight: Maintaining a weight somewhat above your lowest medication-assisted weight but below your starting weight still provides health benefits. Perfect should not be the enemy of good.
Building your maintenance foundation now
Every day of GLP-1 treatment offers an opportunity to prepare for life without medication. The habits you build, the skills you develop, and the relationship with food you establish all transfer to maintenance.
This process works best as an intentional part of treatment rather than a last-minute scramble. Consider working with a registered dietitian who can help develop sustainable eating patterns. Establish an exercise routine that does not depend on medication-enhanced energy. Address emotional eating through therapy or structured programs if needed.
The comprehensive approach to nutrition during GLP-1 therapy outlined in our complete guide to GLP-1 nutrition provides the foundation. Maintenance simply continues what treatment begins.
The medication opened a door. Walking through it and building something lasting remains your responsibility. What specific habits are you developing now that will support you after treatment ends?