





The headache arrived around 2pm, a dull throb that Advil barely touched. By evening, the fatigue had set in, that heavy, dragging exhaustion that made even simple tasks feel monumental. The assumption was obvious: another Ozempic side effect to push through.
Except it was not a medication side effect. It was dehydration, plain and simple. And it had been building for weeks without recognition.
This scenario plays out repeatedly among GLP-1 medication users. The same appetite suppression that reduces food intake also diminishes thirst signals. Water consumption drops without conscious awareness. Electrolyte balance shifts as eating patterns change. And symptoms that get attributed to the medication itself often trace back to something far more correctable. This is precisely why hydration cannot be treated as an afterthought, it sits within a broader nutritional framework that determines how well you tolerate and respond to treatment. The complete guide to nutrition while taking GLP-1 medications addresses every layer of that framework, from protein and fiber to fluids and micronutrients.
Hydration may be the most overlooked aspect of GLP-1 nutrition, yet addressing it often produces the most immediate improvement in how users feel.
GLP-1 receptor agonists are a class of injectable medications originally developed to treat type 2 diabetes. They mimic glucagon-like peptide-1, a natural hormone that regulates blood sugar, slows gastric emptying, and signals fullness to the brain.
Because they significantly reduce appetite, several GLP-1 medications are now FDA-approved for chronic weight management in adults with obesity or overweight with related health conditions.
Common examples: Ozempic and Wegovy (semaglutide), Mounjaro and Zepbound (tirzepatide), Saxenda (liraglutide), and Trulicity (dulaglutide).
Why dehydration risk increases on GLP-1 therapy
Multiple factors converge to increase dehydration risk during GLP-1 treatment, creating a challenge that requires active management rather than passive awareness.
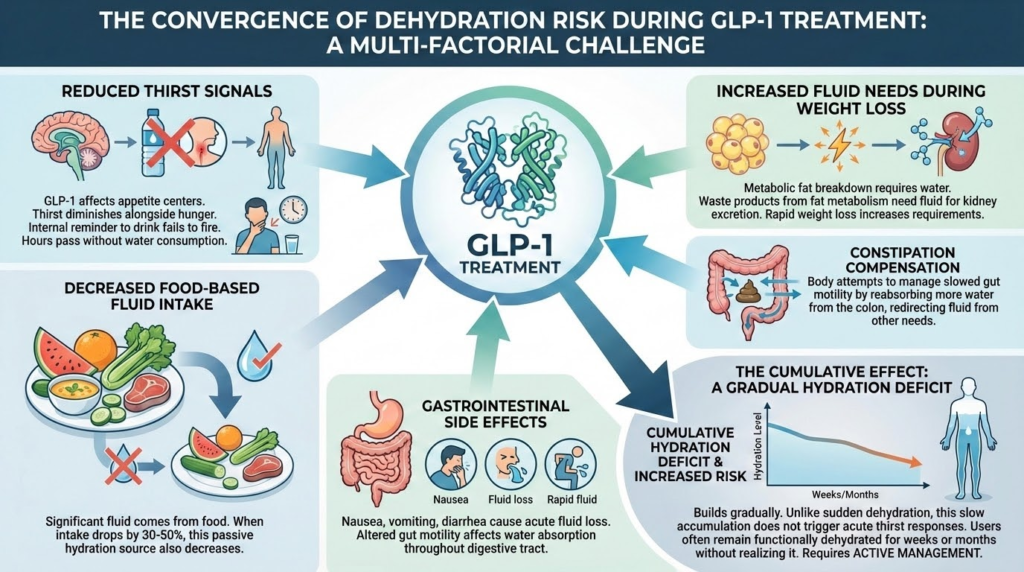
Reduced thirst signals: GLP-1 receptor agonists affect appetite centers in the brain, and for many users, thirst diminishes alongside hunger. The internal reminder to drink simply does not fire with normal frequency. Hours pass without water consumption because the body never signals its need.
Decreased food-based fluid intake: A surprising amount of daily fluid comes from food rather than beverages. Fruits, vegetables, soups, and even meat contain significant water content. When food intake drops by 30 to 50 percent, so does this passive hydration source.
Gastrointestinal side effects: Nausea, vomiting, and diarrhea during dose titration can cause acute fluid loss. Even without these dramatic symptoms, altered gut motility affects water absorption throughout the digestive tract.
Increased fluid needs during weight loss: The metabolic processes involved in breaking down fat tissue require water. Waste products from fat metabolism need fluid for kidney excretion. Rapid weight loss actually increases hydration requirements at precisely the time intake tends to drop.
Constipation compensation: The body attempts to manage slowed gut motility by reabsorbing more water from the colon. This helps with stool formation but redirects fluid away from other needs.
The cumulative effect is a hydration deficit that builds gradually. Unlike sudden dehydration from exercise or heat exposure, this slow accumulation does not trigger acute thirst responses. Users often remain functionally dehydrated for weeks or months without realizing it.
Recognizing dehydration symptoms
Dehydration symptoms overlap substantially with commonly reported GLP-1 side effects, making identification tricky. Many users accept these symptoms as medication consequences when hydration could resolve them.
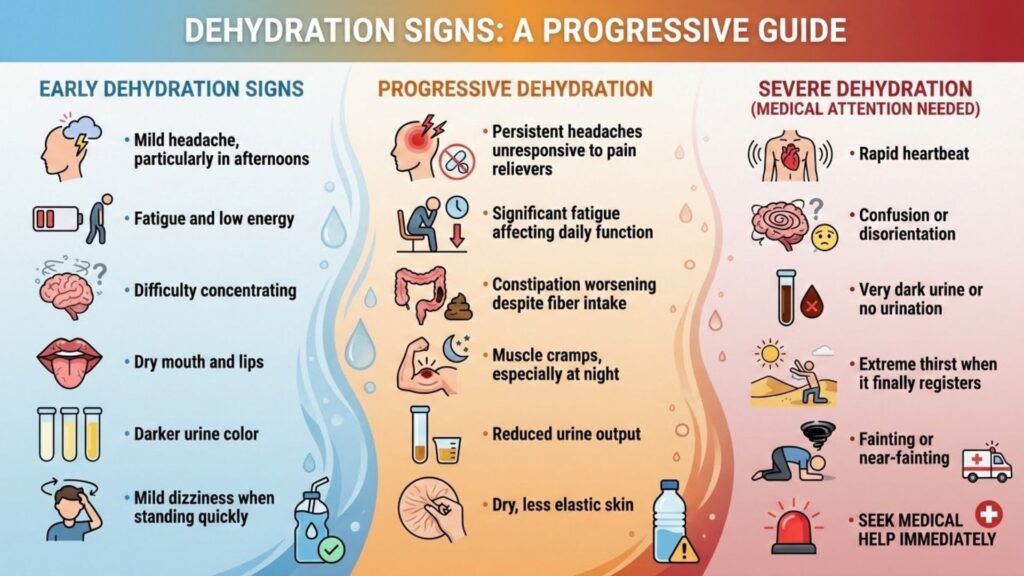
The simplest diagnostic test requires no equipment: check your urine color. Pale yellow to clear indicates adequate hydration. Dark yellow or amber signals dehydration requiring immediate attention. This single observation provides more useful information than any symptom checklist.
How much fluid do GLP-1 users need?
Standard recommendations suggest eight 8-ounce glasses of water daily, approximately 64 ounces or 2 liters. For GLP-1 users, this represents a minimum rather than a target.
More personalized guidance calculates fluid needs based on body weight. A common formula suggests half an ounce to one ounce of water per pound of body weight daily. For a 180-pound person, this translates to 90 to 180 ounces, a substantial range that accounts for activity level, climate, and individual variation.
Given the increased dehydration risk during GLP-1 therapy, aiming toward the higher end of this range makes sense for most users. A practical target of 80 to 100 ounces daily works well for average-sized adults during active treatment.
This sounds like a lot because it is. Meeting these targets requires intentional effort throughout the day. Waiting for thirst to prompt drinking virtually guarantees inadequate intake.
Practical hydration strategies
Knowing you need to drink more and actually doing it are different challenges. These strategies help bridge the gap between intention and execution.
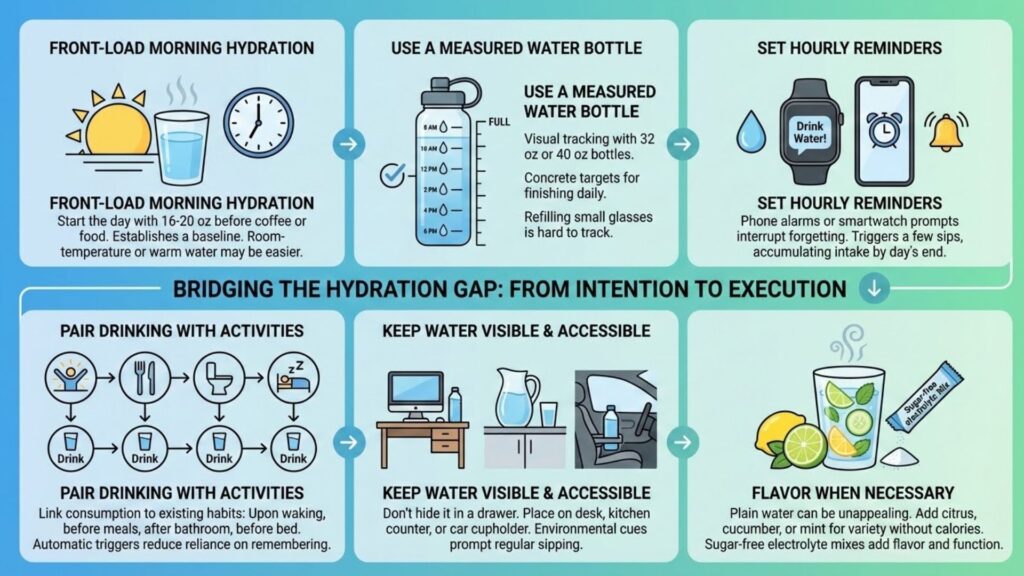
Front-load morning hydration: Start each day with 16 to 20 ounces of water before coffee, food, or anything else. This establishes a baseline that reduces the catch-up required later. Many users find room-temperature or warm water easier to consume first thing than cold.
Use a measured water bottle: A 32-ounce or 40-ounce bottle with time markers provides visual tracking and clear goals. Knowing you need to finish the bottle twice or three times daily creates concrete targets. Refilling a small glass repeatedly makes tracking nearly impossible.
Set hourly reminders: Phone alarms or smartwatch prompts every hour interrupt the pattern of forgetting to drink. Each reminder triggers a few sips, accumulating substantial intake by day’s end.
Pair drinking with activities: Link water consumption to existing habits. Drink a full glass upon waking, before each meal, after using the bathroom, and before bed. These automatic triggers reduce reliance on remembering.
Keep water visible and accessible: A water bottle that sits in a drawer gets ignored. One that sits on your desk, kitchen counter, or car cupholder prompts regular sipping. Environmental cues matter more than willpower.
Flavor when necessary: Plain water becomes unappealing for some GLP-1 users. Adding lemon, lime, cucumber, or mint provides variety without calories. Sugar-free electrolyte mixes add both flavor and functional benefits.
Understanding electrolyte balance
Water alone does not fully address hydration. Electrolytes, the minerals that conduct electrical signals throughout the body, must remain in balance for proper fluid distribution and cellular function.
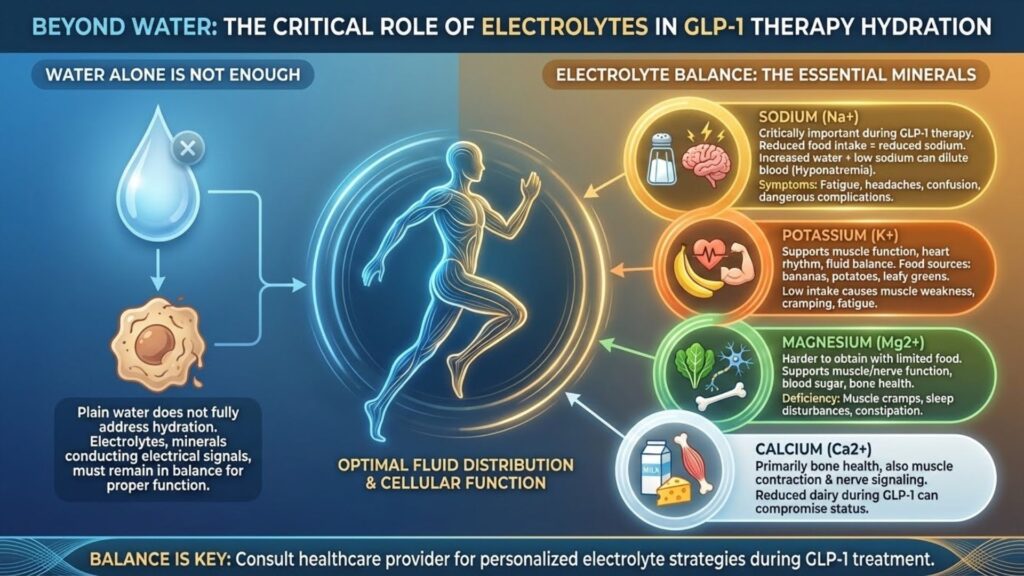
The primary electrolytes of concern include:
Sodium: Often demonized in general nutrition advice, sodium becomes critically important during GLP-1 therapy. Reduced food intake means reduced sodium intake. Combined with increased water consumption, this can dilute blood sodium levels, causing a condition called hyponatremia that produces fatigue, headaches, confusion, and in severe cases, dangerous complications.
Potassium: This mineral supports muscle function, heart rhythm, and fluid balance. Food sources like bananas, potatoes, and leafy greens provide most dietary potassium, and reduced eating limits intake. Low potassium causes muscle weakness, cramping, and fatigue.
Magnesium: Already commonly deficient in the general population, magnesium becomes harder to obtain through limited food intake. It supports muscle and nerve function, blood sugar regulation, and bone health. Deficiency contributes to muscle cramps, sleep disturbances, and constipation.
Calcium: While primarily associated with bone health, calcium also plays roles in muscle contraction and nerve signaling. Reduced dairy intake during GLP-1 therapy can compromise calcium status.
Electrolyte supplementation approaches
Several strategies help maintain electrolyte balance during GLP-1 treatment.
Electrolyte drinks and powders: Products like LMNT, Drip Drop, Liquid IV, and Nuun provide electrolytes in convenient formats. Look for options low in sugar or sugar-free. Many GLP-1 users find these more palatable than plain water and more likely to actually consume.
Sodium from food sources: When appetite allows, incorporating naturally sodium-rich foods helps. Bone broth provides sodium along with collagen and other nutrients. Pickles, olives, and salted nuts offer sodium in small, tolerable portions. For those who can manage it, lightly salting food supports sodium intake.
Salt supplementation: Some users add a pinch of high-quality salt (sea salt or Himalayan pink salt) directly to water. This provides sodium without the sweeteners present in many electrolyte products. Start with small amounts to assess taste tolerance.
Magnesium supplements: Given widespread deficiency and the challenges of food-based intake, magnesium supplementation makes sense for most GLP-1 users. Magnesium glycinate or citrate forms absorb well and rarely cause digestive upset. Doses of 200 to 400 mg daily address most needs.
Potassium considerations: Potassium supplementation requires more caution than other electrolytes. Over-the-counter supplements are limited to low doses by regulation because excess potassium poses cardiac risks. Focus on food sources when possible, and discuss supplementation with your healthcare provider if concerned about deficiency.
A daily hydration protocol
Translating principles into practice, here is a sample daily hydration framework:
| Time | Action | Volume |
| Upon waking | Water with lemon or plain | 16–20 oz |
| Mid-morning | Water or electrolyte drink | 16 oz |
| Before lunch | Water | 8–12 oz |
| Afternoon | Electrolyte drink or water with salt | 16–20 oz |
| Before dinner | Water | 8–12 oz |
| Evening | Herbal tea or water | 12–16 oz |
| Before bed | Small amount of water | 4–8 oz |
| Daily total | 80–100 oz |
Adjustments based on activity level, climate, and individual needs keep this framework flexible. Hot weather, exercise, or GI symptoms all increase requirements.
Beverages that count and those that do not
Not all fluids contribute equally to hydration status.
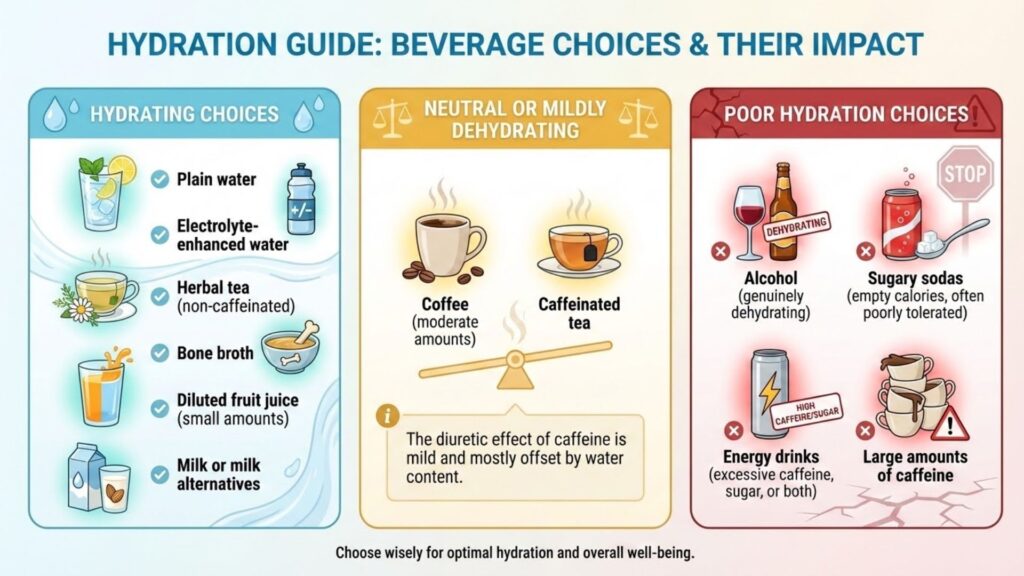
Coffee deserves specific mention because many GLP-1 users rely on it for energy. Moderate coffee consumption, two to three cups daily, does not significantly impair hydration for most people. The water content roughly balances the mild diuretic effect. However, coffee should not replace water as the primary fluid source.
Hydration and other GLP-1 challenges
Proper hydration connects to nearly every other nutritional challenge during GLP-1 therapy.
Constipation improves substantially with adequate fluid intake. Fiber without water creates concrete rather than soft, passable stool. The strategies outlined in our article on fiber and gut health work best when hydration is simultaneously addressed.
Energy levels stabilize when dehydration is eliminated as a contributing factor. Fatigue attributed to the medication or to caloric restriction often resolves with improved fluid intake.
Headaches that seemed like inevitable side effects frequently disappear with consistent hydration. This alone can dramatically improve quality of life during treatment.
Kidney function depends on adequate fluid for processing the metabolic byproducts of weight loss. Supporting kidney health through hydration may reduce other complications over long-term treatment.
These interconnections are explored comprehensively in our complete guide to GLP-1 nutrition, where hydration takes its place alongside protein, fiber, and micronutrient strategies.
Sometimes the simplest interventions produce the most profound improvements. Before attributing symptoms to medication side effects or treatment complications, what happens when you consistently drink enough water for two weeks? Hydration is often the lowest-hanging fruit, but for those who have addressed it and still struggle, targeted supplementation can fill the remaining gaps. The guide to the best supplements for GLP-1 and Ozempic users identifies exactly which supplements are worth taking, which are overhyped, and how to prioritize them based on your specific symptoms.