




The before-and-after photos flooding social media tell only half the story. Yes, the weight came off. But look closer at some of those transformations and you will notice something troubling: saggy skin, hollow cheeks, thin arms, and a frail appearance that suggests the body lost far more than just fat.
This is the hidden cost of rapid weight loss that the GLP-1 medication conversation has been slow to address. Clinical data from semaglutide trials reveals that approximately 39% of total weight lost came from lean mass rather than adipose tissue. For someone losing 50 pounds, that potentially means 20 pounds of muscle, bone density, and connective tissue gone alongside the fat.
The good news? Muscle loss on GLP-1 medications is largely preventable. But it requires deliberate action that goes beyond simply taking your weekly injection and eating less.
GLP-1 receptor agonists are a class of injectable medications originally developed to treat type 2 diabetes. They mimic glucagon-like peptide-1, a natural hormone that regulates blood sugar, slows gastric emptying, and signals fullness to the brain.
Because they significantly reduce appetite, several GLP-1 medications are now FDA-approved for chronic weight management in adults with obesity or overweight with related health conditions.
Common examples: Ozempic and Wegovy (semaglutide), Mounjaro and Zepbound (tirzepatide), Saxenda (liraglutide), and Trulicity (dulaglutide).
Understanding why GLP-1 drugs cause muscle loss
Your body does not distinguish between intentional weight loss and starvation. When caloric intake drops dramatically, as it does for most GLP-1 users, the body enters a catabolic state. It begins breaking down tissue to meet energy demands and maintain blood sugar levels.
Fat tissue gets mobilized, which is the desired outcome. But muscle tissue also gets sacrificed, particularly when two conditions exist: insufficient protein intake and lack of mechanical stimulus telling the body that muscles are needed.
GLP-1 medications create a perfect storm for muscle loss. Appetite suppression leads to reduced protein consumption. Fatigue during the titration phase discourages physical activity. Rapid weight loss outpaces the body’s ability to adapt. And the older you are, the more pronounced these effects become.
The phenomenon has grown common enough to earn its own terminology. “Ozempic body” describes the deflated, loose-skinned appearance that develops when someone loses substantial weight without preserving underlying muscle structure. “Ozempic face” refers to facial volume loss that can add years to someone’s appearance despite significant weight reduction.
The real numbers: how much muscle are people losing?
The STEP 1 trial, which led to Wegovy’s FDA approval, documented body composition changes using DEXA scanning. Participants lost an average of 14.9% of their body weight over 68 weeks. Of that weight loss, approximately 39% came from lean mass.
To put this in perspective: a 200-pound person losing 30 pounds on semaglutide might lose nearly 12 pounds of muscle and only 18 pounds of fat under typical conditions.
The SELECT cardiovascular outcomes trial and subsequent studies have shown similar patterns. Without intervention, GLP-1 induced weight loss consistently sacrifices lean tissue at rates that exceed what researchers consider acceptable for healthy weight management.
Compare this to well-designed weight loss protocols that incorporate resistance training and adequate protein. These approaches typically limit lean mass loss to 15 to 25% of total weight lost. The difference matters enormously for long-term metabolic health and physical function.
Why preserving muscle matters beyond appearance
Vanity concerns aside, muscle tissue serves critical metabolic and functional purposes that extend far beyond looking fit.
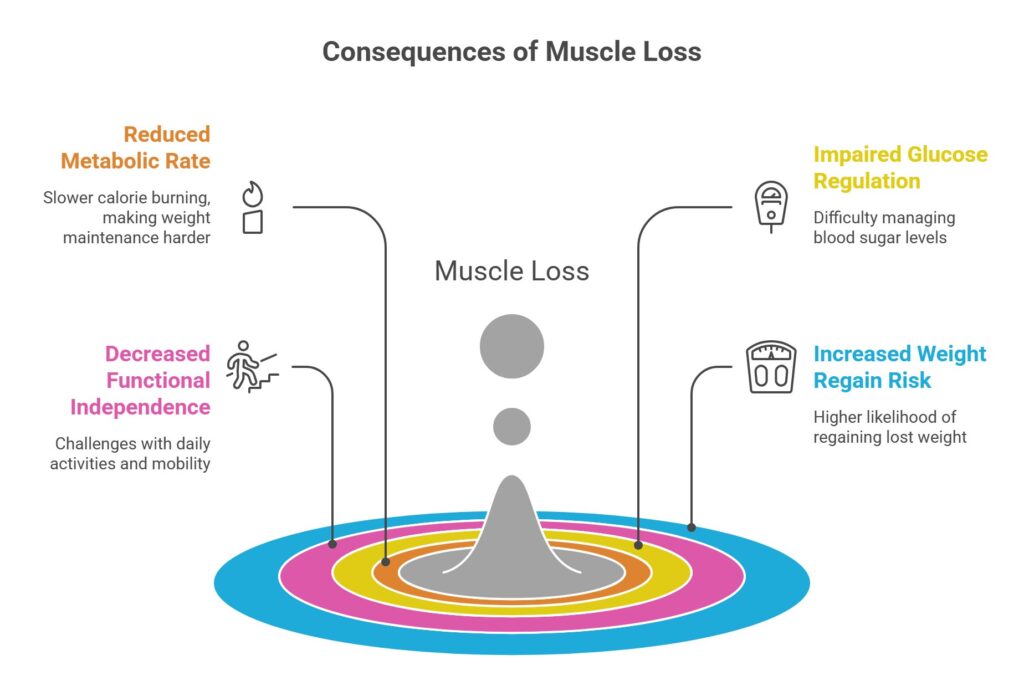
Metabolic rate: Muscle is metabolically active tissue that burns calories even at rest. Each pound of muscle burns approximately 6 to 10 calories daily just to maintain itself. Lose 15 pounds of muscle and your resting metabolism drops by 90 to 150 calories per day. This creates a significant headwind for long-term weight maintenance.
Glucose regulation: Skeletal muscle serves as the primary site for glucose disposal after meals. Less muscle means less capacity to clear blood sugar efficiently. Ironically, losing too much muscle while treating obesity can worsen the insulin resistance that often accompanies excess weight.
Functional independence: For adults over 50, muscle loss accelerates age-related decline in strength and mobility. Falls, fractures, difficulty climbing stairs, and loss of independence all correlate with reduced muscle mass. GLP-1 induced muscle loss can effectively age someone’s functional capacity by years.
Weight regain risk: Perhaps most concerning, muscle loss makes weight regain more likely. A slower metabolism requires fewer calories to maintain weight. When GLP-1 therapy ends or appetite returns, the caloric surplus needed to regain weight becomes smaller. Many people regain fat but not the muscle they lost, ending up with worse body composition than before treatment.
The two-pillar strategy for muscle preservation
Preventing muscle loss on GLP-1 medications requires addressing both inputs the body needs to maintain lean tissue: adequate protein and mechanical loading through resistance exercise. Neither alone is sufficient. Both together can dramatically shift the ratio of fat to muscle lost.
Pillar one: protein optimization
Research consistently shows that higher protein intakes during weight loss preserve more lean mass. For GLP-1 users, this means consuming 1.2 to 1.6 grams of protein per kilogram of body weight daily, spread across multiple eating occasions.
This presents a practical challenge when appetite has largely disappeared. Most GLP-1 users struggle to eat 1,200 calories daily, let alone hit protein targets of 100+ grams. Strategic prioritization becomes essential.
Protein must come first at every meal. Before vegetables, before carbohydrates, before fats. The protein on your plate gets eaten completely even if everything else remains. Protein shakes and supplements bridge gaps when whole food consumption falls short.
For detailed guidance on protein targets and food sources, our article on protein needs for Ozempic users provides comprehensive recommendations.
Pillar two: resistance training
Mechanical loading tells your body that muscles are needed. Without this signal, the body has no reason to prioritize muscle preservation over energy conservation.
Resistance training does not require a gym membership or heavy weights. It requires consistent progressive overload, meaning gradually increasing the challenge your muscles face over time.
Two to three resistance training sessions per week, targeting all major muscle groups, provides sufficient stimulus for most people. Each session can be completed in 30 to 45 minutes. Exercises should include movements for legs, back, chest, shoulders, and arms.
For beginners or those returning to exercise after a long break, bodyweight exercises or resistance bands offer an accessible starting point. Push-ups, squats, lunges, rows, and planks require no equipment and can be modified for any fitness level.
The key is consistency and progression. Start with manageable resistance and volume, then gradually increase over weeks and months. Your muscles adapt to the demands you place on them.
A practical weekly framework
Implementing both pillars requires realistic planning. Here is a framework that works for most GLP-1 users:
| Day | Focus | Time Required |
| Monday | Resistance training: Upper body | 30–40 minutes |
| Tuesday | Light activity: Walking, stretching | 20–30 minutes |
| Wednesday | Resistance training: Lower body | 30–40 minutes |
| Thursday | Light activity or rest | As needed |
| Friday | Resistance training: Full body | 30–45 minutes |
| Saturday | Active recovery: Walking, yoga | 20–30 minutes |
| Sunday | Rest | — |
Protein targets remain consistent daily: minimum 1.2 grams per kilogram of body weight, ideally 1.4 to 1.6 grams for those actively training.
Managing energy levels during exercise
Many GLP-1 users report fatigue, particularly during the dose escalation phase. Low energy can make exercise feel impossible. Several strategies help:

Timing matters. Schedule workouts when energy tends to be highest, often in the morning before appetite suppression fully kicks in or on days when side effects are milder.
Pre-workout nutrition. A small protein-rich snack 60 to 90 minutes before training can provide energy without triggering nausea. Greek yogurt, a few bites of chicken, or a partial protein shake often work well.
Adjust expectations. During titration or on high side-effect days, a lighter workout beats no workout. Even a 15-minute resistance session provides muscle-preserving stimulus.
Stay hydrated. Dehydration worsens fatigue. GLP-1 users often under-consume fluids due to reduced thirst signals. Prioritize water intake, especially around exercise.
When professional guidance helps
Working with qualified professionals can accelerate results and prevent injury. A registered dietitian experienced with GLP-1 patients can help structure eating plans that hit protein targets despite reduced appetite. A certified personal trainer can design resistance programs appropriate for your current fitness level and goals.
For those with significant weight to lose or existing health conditions, medical supervision of exercise programming adds an important safety layer. Many obesity medicine clinics now incorporate exercise physiologists and dietitians into their GLP-1 treatment protocols.
The long-term perspective
Muscle preservation during GLP-1 therapy is not just about looking better at your goal weight. It is about arriving at that weight with a functional, metabolically healthy body capable of maintaining results long-term.
The choices you make during active weight loss determine the body composition you live with afterward. Two people can lose identical amounts of weight and end up with dramatically different outcomes depending on how much muscle they preserved along the way.
Starting resistance training and prioritizing protein from the beginning of GLP-1 therapy yields better results than trying to rebuild lost muscle later. Muscle is easier to preserve than to regain, especially as we age.
For a comprehensive understanding of nutritional strategies that support your GLP-1 treatment, our complete guide to nutrition on GLP-1 medications covers protein, fiber, micronutrients, and meal planning in detail.
The medication handles appetite. The rest is up to you. What steps are you taking to protect your muscle mass while the weight comes off?