




The plate sits in front of you, a portion that would have seemed laughably small six months ago. Now it looks overwhelming. Three bites in and you are done, pushing food around while your dinner companions continue eating normally. The disconnect between what you know you should eat and what your body will accept has become the central tension of every meal.
This is the reality of eating on GLP-1 medications that no one adequately prepares you for. The appetite suppression works exactly as advertised, perhaps too well. Food loses its appeal. Portions that once disappeared effortlessly now sit untouched. And somewhere in this dramatic shift, you need to figure out how to actually nourish your body with dramatically reduced intake.
Meal planning on Ozempic, Wegovy, or Mounjaro requires abandoning everything you thought you knew about eating and rebuilding from the ground up.
GLP-1 receptor agonists are a class of injectable medications originally developed to treat type 2 diabetes. They mimic glucagon-like peptide-1, a natural hormone that regulates blood sugar, slows gastric emptying, and signals fullness to the brain.
Because they significantly reduce appetite, several GLP-1 medications are now FDA-approved for chronic weight management in adults with obesity or overweight with related health conditions.
Common examples: Ozempic and Wegovy (semaglutide), Mounjaro and Zepbound (tirzepatide), Saxenda (liraglutide), and Trulicity (dulaglutide).
How GLP-1 medications change your relationship with food
Understanding the physiological changes happening in your body helps explain why old eating patterns no longer work.
GLP-1 receptor agonists slow gastric emptying significantly. Food that previously cleared your stomach in two to three hours may now linger for four to six hours or longer. This prolonged stomach fullness triggers satiety signals that persist far beyond normal duration.
The medications also act directly on appetite centers in the brain, reducing hunger hormones and diminishing the psychological drive to eat. Many users report that food simply stops occupying mental space. The constant background hum of thinking about meals, snacks, and cravings goes quiet.
Additionally, taste perception often shifts. Foods that once brought pleasure may taste different, less appealing, or actively unpleasant. Sweet foods frequently become cloying. Rich, fatty foods can trigger nausea. These changes are not psychological. They reflect genuine alterations in how your nervous system processes taste and satiety signals.
The combined effect is a fundamental transformation in eating behavior. Meals become smaller. Frequency often decreases. Food choices narrow to whatever the body will accept on any given day.
The nutrient density imperative
When you can only eat 1,000 to 1,200 calories daily, every bite must count. There is no room for empty calories, filler foods, or nutritional dead ends. The concept of nutrient density, the amount of vitamins, minerals, protein, and fiber per calorie, becomes the organizing principle of all food choices.
A 200-calorie snack of crackers provides minimal protein, negligible fiber, and few micronutrients. The same 200 calories from Greek yogurt with berries delivers 15 grams of protein, fiber, calcium, probiotics, and antioxidants. The caloric cost is identical. The nutritional return differs enormously.
This shift in thinking applies to every eating decision. Before taking a bite, ask: what is this food actually providing beyond calories? If the answer is not much, that food probably should not occupy your limited stomach real estate.
Practically, this means prioritizing:
- Lean proteins at every eating occasion
- Vegetables and fruits with high fiber-to-sugar ratios
- Whole grains in modest portions when tolerated
- Healthy fats from sources like avocado, nuts, and olive oil
- Minimal added sugars, refined carbohydrates, and ultra-processed foods
Structuring your eating: two meals versus three
The traditional three-meals-plus-snacks pattern rarely works for GLP-1 users. Most find they can only manage two substantial eating occasions daily, sometimes supplemented by a small snack or protein shake.

This is not a problem to solve. It is an adaptation to accept. Forcing yourself to eat three full meals when your body signals fullness after two creates unnecessary discomfort and can worsen nausea.
Two-meal pattern: Many users naturally gravitate toward a late breakfast or brunch and an early dinner, with perhaps a small protein-rich snack in between if needed. This pattern allows adequate time for the stomach to empty between meals and concentrates eating during hours when appetite tends to be slightly stronger.
Three small meals pattern: Some users prefer spreading intake across three very small meals. This can work well for those who experience blood sugar fluctuations or need consistent medication timing with food. Portions at each meal will be quite small, perhaps 300 to 400 calories.
Intermittent eating: A subset of GLP-1 users finds they can only eat during a narrow window, perhaps four to six hours daily. This accidental intermittent fasting is not harmful for most people and may align well with how the medication affects hunger patterns.
The best pattern is whatever allows you to meet minimum protein and nutrient targets while respecting your body’s dramatically altered hunger signals. Experimentation during the first months of treatment helps identify what works for your individual response.
Meal timing considerations
When you eat matters alongside what you eat. Several timing principles help optimize nutrition and minimize side effects during GLP-1 therapy.
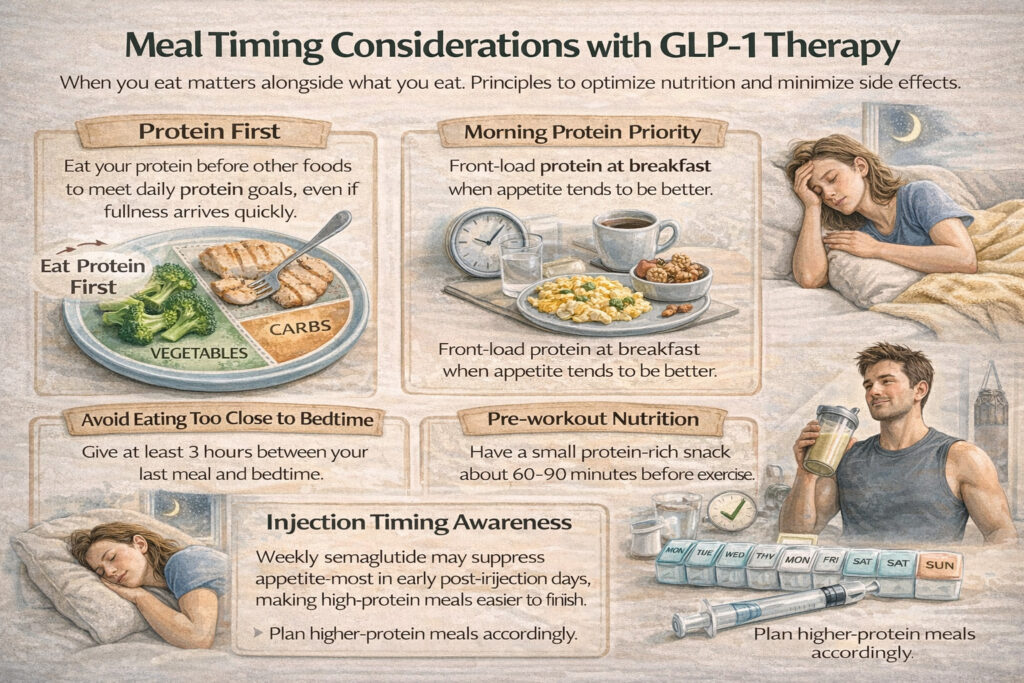
Protein first: At every eating occasion, consume protein before other foods. This ensures you meet protein minimums even if you cannot finish everything on your plate. Starting with vegetables or carbohydrates and saving protein for last often results in inadequate protein intake when fullness arrives early.
Morning protein priority: Many users report that appetite, while still suppressed, tends to be slightly better in the morning hours. Front-loading protein at breakfast or brunch can help hit daily targets. A 30-gram protein breakfast creates a substantial cushion even if later meals fall short.
Avoid eating too close to bedtime: Slowed gastric emptying means food consumed late in the evening may not clear the stomach before you lie down. This increases reflux risk and can disrupt sleep. Aim to finish eating at least three hours before bed.
Injection timing awareness: If you use weekly semaglutide, you may notice stronger appetite suppression in the days immediately following injection versus the end of the week. Some users strategically plan higher-protein meals for days when eating feels slightly easier.
Pre-workout nutrition: If you exercise, consuming a small protein-rich snack 60 to 90 minutes before training provides energy without triggering nausea. Liquid nutrition like a partial protein shake often works better than solid food close to exercise.
Practical portion guidance
Portions that made sense before GLP-1 therapy will likely be too large now. Recalibrating expectations prevents food waste and the psychological frustration of consistently leaving half-finished plates.
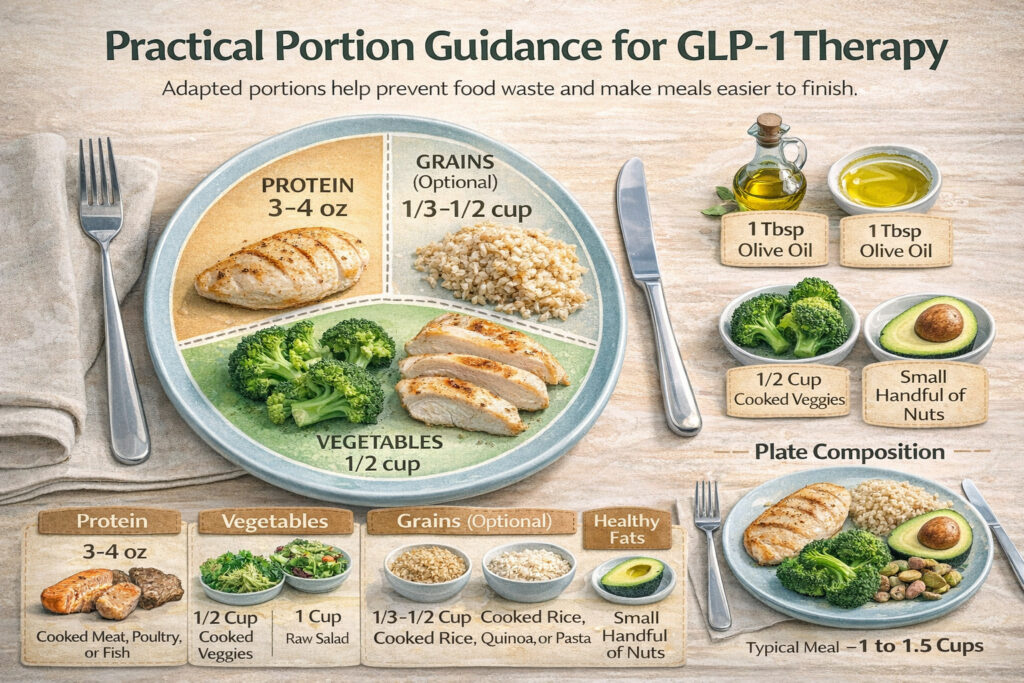
Protein portions: Aim for 3 to 4 ounces of cooked meat, poultry, or fish per meal rather than the 6 to 8 ounces typical in American portions. This smaller portion delivers 21 to 28 grams of protein, a meaningful amount that most GLP-1 users can finish.
Vegetable portions: Half to one cup of cooked vegetables or one to two cups of raw salad represents a realistic serving. Choose vegetables you actually enjoy since forcing down large volumes rarely works.
Grain portions: If including grains, one-third to one-half cup of cooked rice, quinoa, or pasta provides fiber and energy without excessive bulk. Some users eliminate grains entirely to save stomach space for protein and vegetables.
Fat portions: Healthy fats add necessary calories in small volumes. One tablespoon of olive oil, one-quarter of an avocado, or a small handful of nuts contributes meaningful nutrition without requiring significant stomach capacity.
Total plate composition: A typical meal might include 3 to 4 ounces of protein, half a cup of vegetables, and a small portion of healthy fat. Total volume is perhaps one to one and a half cups of food, dramatically less than a standard American meal.
Sample meal frameworks
Concrete examples help translate principles into practice. These frameworks provide starting points to customize based on individual tolerance and preferences.
Framework 1: two meals plus protein shake
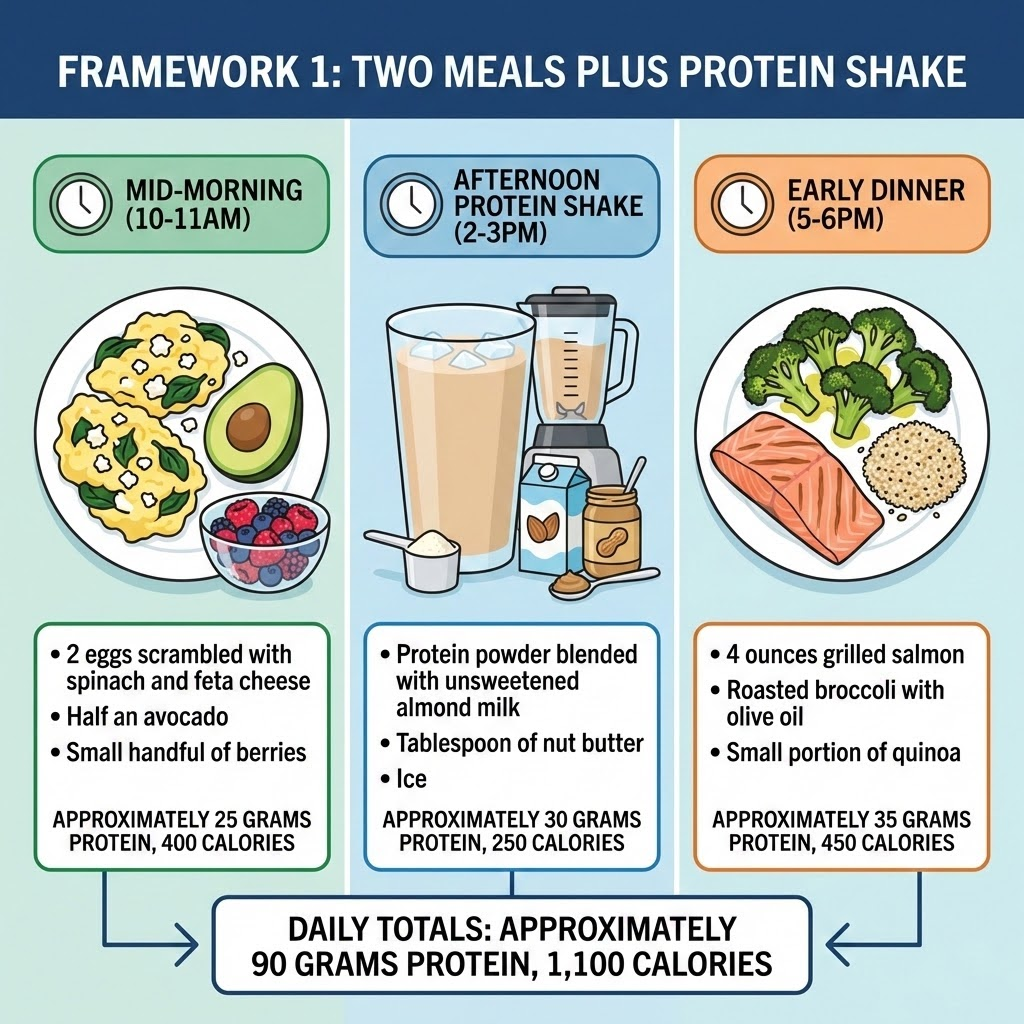
This pattern works well for users who wake without appetite but can manage food by mid-morning. The protein shake bridges the gap between meals without requiring a full eating session, making it easier to hit protein targets when solid food feels overwhelming.
Notice how protein is distributed across all three eating occasions rather than concentrated at dinner. This spacing supports steady amino acid availability for muscle preservation throughout the day. The mid-morning meal anchors the day with eggs and healthy fats, the shake delivers efficient protein with minimal volume, and dinner closes with nutrient-dense whole foods.
The calorie total may look low compared to pre-medication intake, but this often matches what GLP-1 users can comfortably consume. If energy levels drop or hunger increases on certain days, adding a small handful of nuts or an extra tablespoon of nut butter to the shake provides a quick adjustment without requiring another full meal.
Framework 2: three small meals
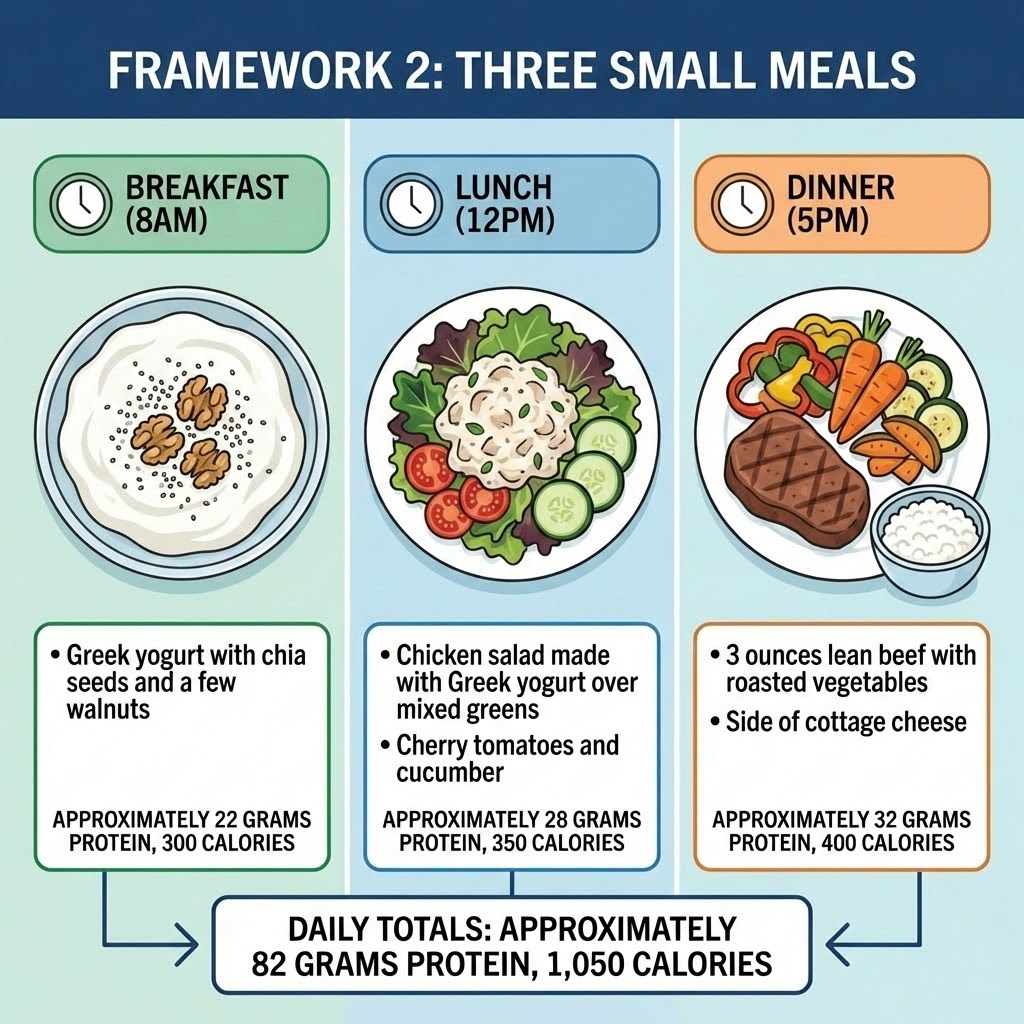
This pattern suits users who prefer consistent eating times or need to take other medications with food throughout the day. Smaller, more frequent meals can also help those who experience blood sugar dips between longer gaps.
The key difference from traditional eating is portion size. Each meal delivers meaningful protein but remains small enough to finish comfortably. Greek yogurt appears twice here intentionally, serving as both a breakfast base and a creamy dressing alternative at lunch, keeping protein high without heavy cooking.
Dinner stays on the lighter side compared to typical evening meals. Many GLP-1 users find digestion slows significantly by late afternoon, so ending the day with a modest plate prevents the discomfort of going to bed with food still sitting heavy.
If 1,050 calories feels too restrictive on active days, the easiest adjustment is adding a small portion of complex carbs to lunch or dinner, such as half a sweet potato or a few tablespoons of quinoa.
Framework 3: one meal plus substantial snacks
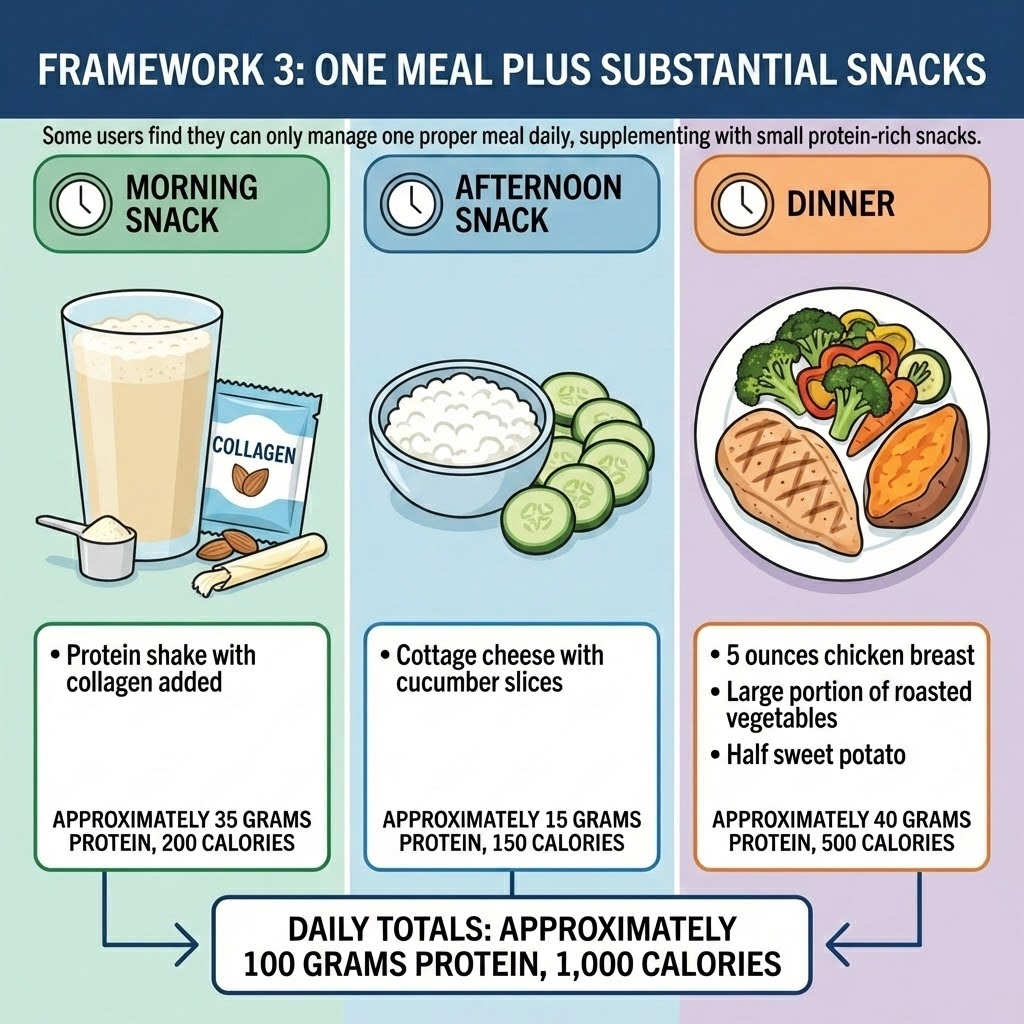
Some users discover that appetite simply does not show up until evening. Fighting this pattern often backfires, leading to forced eating and worsening nausea. This framework embraces the reality by building protein intake around one substantial dinner while using strategic snacks to maintain muscle-protective amino acid levels throughout the day.
The protein shake with added collagen serves double duty, delivering protein while supporting skin elasticity that can become a concern during rapid weight loss. Cottage cheese mid-afternoon requires zero preparation and digests easily for most users. These are not meals disguised as snacks but genuinely small, functional doses of nutrition.
Dinner carries the heaviest lifting here, both in protein and overall satisfaction. A larger portion of vegetables fills the plate visually and provides fiber without excessive calories. The optional evening snack exists for days when hunger resurfaces or when the day’s protein total needs a small boost.
This pattern often emerges naturally during higher doses of medication. Rather than viewing it as a problem, many users find it simplifies their day while still hitting nutritional targets.
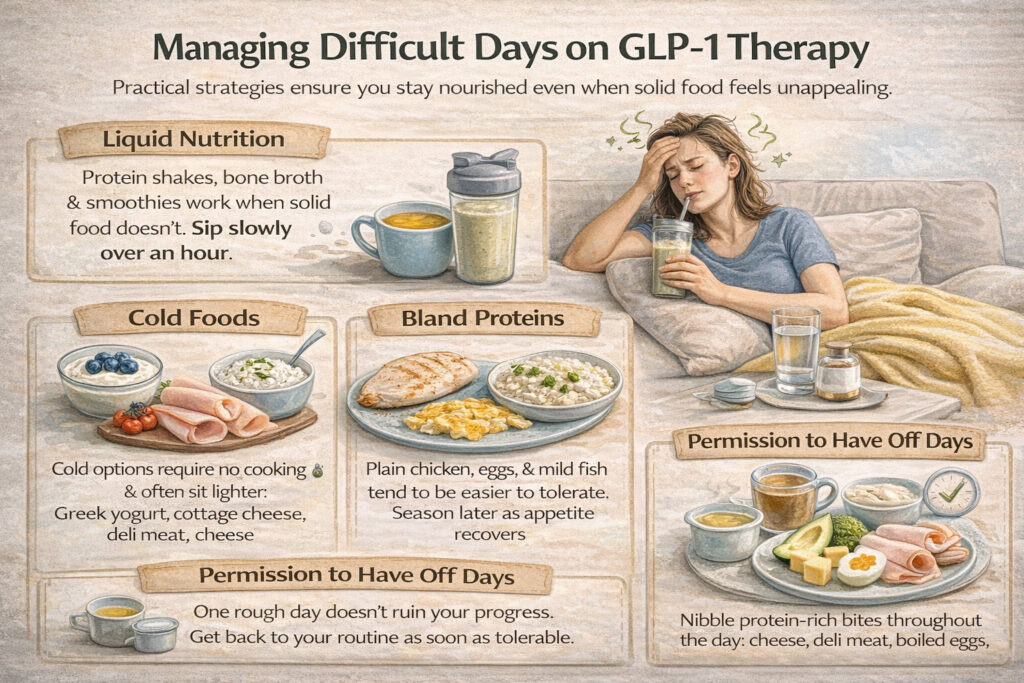
Managing difficult days
Not every day will go smoothly. Nausea flares, food aversions intensify, and sometimes nothing sounds remotely appealing. Having strategies for difficult days prevents complete nutritional collapse.
Liquid nutrition: When solid food feels impossible, protein shakes, bone broth, and smoothies provide nutrition in more tolerable formats. Sipping slowly over an hour often works better than attempting to drink quickly.
Cold foods: Many GLP-1 users find cold or room-temperature foods easier to tolerate than hot meals. Greek yogurt, cottage cheese, deli meat, cheese, and chilled chicken require no cooking and sit lighter in the stomach.
Bland proteins: Unseasoned chicken, plain eggs, and mild fish often work when more flavorful options trigger aversion. Seasoning can be added later as tolerance improves.
Small frequent bites: Rather than sitting down to a meal, some users do better grazing on protein-rich bites throughout the day. A few cubes of cheese here, a couple bites of chicken there, accumulating protein gradually.
Permission to have off days: Occasionally, despite best efforts, intake will fall short. One difficult day does not derail overall progress. Return to normal eating patterns as soon as tolerable rather than attempting to compensate by overeating.
Building sustainable habits
The eating patterns you establish during GLP-1 therapy become the foundation for long-term weight maintenance. Developing genuine enjoyment of nutrient-dense foods, learning appropriate portion sizes, and understanding your body’s true hunger signals all contribute to lasting success.
These practical meal strategies work alongside the other nutritional priorities covered in our complete guide to GLP-1 nutrition, including protein optimization, fiber intake, and micronutrient adequacy.
The challenge of eating well on GLP-1 medications is real, but it is solvable. With strategic planning and willingness to experiment, most users find an approach that provides adequate nutrition within their new appetite parameters. What meal timing pattern has worked best for you since starting treatment?