




The supplement aisle has never looked more overwhelming. Rows of bottles promising to enhance your GLP-1 results, prevent side effects, boost energy, and optimize everything from hair growth to metabolism. Influencers hawk their affiliate links. Wellness brands launch GLP-1-specific formulations weekly. Everyone has an opinion on what you absolutely must take.
Most of it is noise. Some of it is genuinely helpful. A small portion could actually cause harm.
Cutting through the marketing to identify supplements that address real nutritional gaps during GLP-1 therapy requires understanding what your body actually needs when food intake drops by half, not what someone trying to sell you something claims you need.
GLP-1 receptor agonists are a class of injectable medications originally developed to treat type 2 diabetes. They mimic glucagon-like peptide-1, a natural hormone that regulates blood sugar, slows gastric emptying, and signals fullness to the brain.
Because they significantly reduce appetite, several GLP-1 medications are now FDA-approved for chronic weight management in adults with obesity or overweight with related health conditions.
Common examples: Ozempic and Wegovy (semaglutide), Mounjaro and Zepbound (tirzepatide), Saxenda (liraglutide), and Trulicity (dulaglutide).
The case for supplementation during GLP-1 therapy
Under normal circumstances, a balanced diet provides most micronutrients healthy adults require. Supplementation becomes a backup plan for specific deficiencies or populations with increased needs.
GLP-1 therapy changes this equation fundamentally.
When caloric intake drops to 1,000 to 1,200 calories daily, meeting micronutrient needs through food alone becomes mathematically improbable regardless of food quality. Even the most nutrient-dense diet falls short when total volume decreases by 40 to 50 percent.
Simultaneously, rapid weight loss increases metabolic demands for certain nutrients. Fat metabolism requires B vitamins. Muscle preservation demands adequate protein and supporting cofactors. Bone density maintenance needs calcium, vitamin D, and magnesium. The body’s requirements do not decrease just because intake has.
Add common GI side effects that further impair nutrient absorption, and supplementation shifts from optional to essential for most GLP-1 users.
This does not mean swallowing handfuls of pills or buying every trendy product marketed to weight loss patients. It means strategic supplementation targeting documented deficiency risks with evidence-based interventions.
Tier 1: essential supplements for most GLP-1 users
These supplements address the most common and consequential nutritional gaps during GLP-1 therapy. Most users benefit from including all of them.
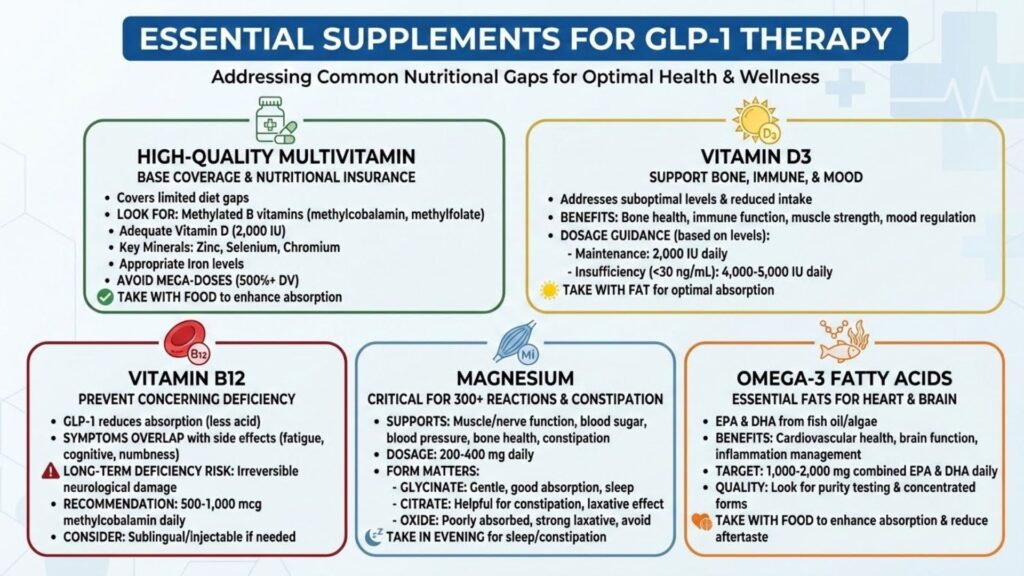
High-quality multivitamin
A comprehensive multivitamin provides baseline coverage across the micronutrient spectrum. Think of it as nutritional insurance that catches gaps your limited diet might miss.
Not all multivitamins are created equal. Look for formulations that include:
- Methylated B vitamins (methylcobalamin for B12, methylfolate for folate) for optimal absorption
- Adequate vitamin D (at least 1,000 IU, preferably 2,000 IU)
- Minerals including zinc, selenium, and chromium
- Appropriate iron levels (women’s formulas typically include more; men’s formulas may exclude iron)
Avoid mega-dose formulations that provide 500% or 1,000% of daily values. More is not better with most micronutrients, and excessive amounts of certain vitamins can cause harm.
Take your multivitamin with food when possible to enhance absorption of fat-soluble vitamins and reduce the nausea some users experience with supplements on an empty stomach.
Vitamin D3
Even with a multivitamin, additional vitamin D supplementation often makes sense. Most Americans have suboptimal vitamin D levels before starting GLP-1 therapy. Reduced food intake, particularly of fortified dairy and fatty fish, pushes levels lower.
Vitamin D supports bone health, immune function, muscle strength, and mood regulation. Deficiency has been linked to increased infection risk, depression, and impaired glucose metabolism, all concerns during weight loss treatment.
Dosing depends on baseline levels, ideally determined through blood testing. General guidance suggests:
- 2,000 IU daily for maintenance in those with adequate levels
- 4,000 to 5,000 IU daily for those with insufficiency (levels below 30 ng/mL)
- Higher doses under medical supervision for frank deficiency
Vitamin D3 (cholecalciferol) absorbs better than D2 (ergocalciferol). Take it with a meal containing some fat for optimal absorption.
Vitamin B12
B12 deficiency emerges as one of the most concerning nutritional consequences of GLP-1 treatment. These medications reduce gastric acid secretion and slow stomach emptying, both of which impair B12 absorption.
Symptoms of B12 deficiency, including fatigue, cognitive changes, numbness, and mood disturbances, overlap with commonly reported medication side effects. This overlap makes deficiency easy to miss without blood testing.
Long-term B12 deficiency causes irreversible neurological damage, making prevention far preferable to treatment.
Supplementation of 500 to 1,000 mcg daily of methylcobalamin (the active form) provides protection for most users. Those with documented deficiency or absorption issues may need higher doses or sublingual/injectable forms that bypass the GI tract.
Adults over 50 and those taking acid-reducing medications alongside GLP-1 therapy face particularly elevated risk and should prioritize B12 supplementation.
Magnesium
Magnesium deficiency affects an estimated 50% of the general American population before any dietary restriction. Reduced food intake during GLP-1 therapy exacerbates this widespread insufficiency.
This mineral supports over 300 enzymatic reactions in the body, including muscle and nerve function, blood sugar regulation, blood pressure control, and bone health. It also helps with constipation, one of the most common GLP-1 complaints.
Supplementation of 200 to 400 mg daily addresses most needs. Form matters:
- Magnesium glycinate: Well-absorbed, gentle on stomach, good for general supplementation and sleep support
- Magnesium citrate: Well-absorbed, more laxative effect, helpful for those with constipation
- Magnesium oxide: Poorly absorbed, strong laxative effect, not recommended for addressing deficiency
- Magnesium threonate: Crosses blood-brain barrier, marketed for cognitive benefits, more expensive
Take magnesium in the evening if using for sleep or constipation support. Split doses if taking more than 200 mg to improve absorption and reduce any GI effects.
Omega-3 fatty acids
Omega-3s from fish oil or algae provide EPA and DHA, essential fatty acids that support cardiovascular health, brain function, and inflammation management. Most Americans consume inadequate omega-3s even with normal eating patterns.
During GLP-1 therapy, fish consumption often decreases due to food aversions or limited eating occasions. Supplementation ensures adequate intake of these essential fats.
Aim for combined EPA and DHA of 1,000 to 2,000 mg daily. Quality matters significantly with fish oil. Look for products tested for purity and freshness, stored appropriately, and providing concentrated EPA/DHA rather than filler oils.
Take omega-3s with food to enhance absorption and reduce any fishy aftertaste or reflux. Refrigerating liquid fish oil improves palatability for some users.
Tier 2: situational supplements based on individual needs
These supplements benefit specific populations or address particular symptoms. Consider based on your individual circumstances.
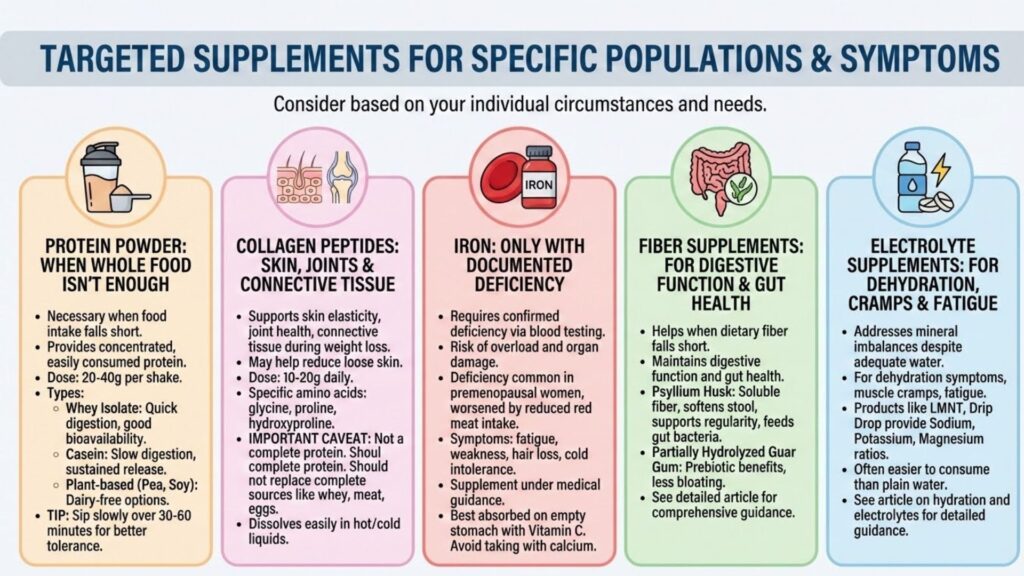
Protein powder
When whole food protein intake falls short despite best efforts, protein supplementation becomes necessary rather than optional. Many GLP-1 users simply cannot eat enough food to meet protein targets through meals alone.
Protein powder provides a concentrated, easily consumed protein source. A single shake can deliver 20 to 40 grams of protein in a format many users find easier to tolerate than solid food.
Whey protein isolate offers excellent bioavailability and amino acid profile. It digests relatively quickly and works well for most users. Those with lactose sensitivity often tolerate isolate better than concentrate.
Casein protein digests more slowly, providing sustained amino acid release. It may work well before bed or when longer satiety is desired.
Plant-based options like pea protein, soy protein, or blended formulations suit those avoiding dairy. Ensure adequate leucine content for muscle protein synthesis support.
Sip protein shakes slowly over 30 to 60 minutes rather than consuming quickly. This improves tolerance and allows the slowed digestive system to process the protein effectively.
Collagen peptides
Collagen supplementation has gained popularity for supporting skin elasticity, joint health, and connective tissue during rapid weight loss. Some evidence suggests collagen may help reduce the loose skin that concerns many GLP-1 users.
Collagen provides specific amino acids (glycine, proline, hydroxyproline) that support connective tissue synthesis. Doses of 10 to 20 grams daily appear in most research showing benefits.
Important caveat: collagen is not a complete protein. It lacks essential amino acids needed for muscle protein synthesis. Collagen should supplement rather than replace complete protein sources like whey, meat, eggs, or dairy.
Collagen dissolves easily in hot or cold liquids and can be added to coffee, smoothies, or other beverages without affecting taste significantly.
Iron
Iron supplementation should only occur with documented deficiency confirmed through blood testing. Unlike water-soluble vitamins where excess is excreted, iron accumulates in the body. Iron overload causes organ damage.
That said, iron deficiency is common, particularly among premenopausal women. Symptoms include fatigue, weakness, hair loss, and cold intolerance. GLP-1 therapy can worsen existing insufficiency through reduced intake of iron-rich foods like red meat.
If testing confirms deficiency, supplementation under medical guidance restores levels. Iron absorbs best on an empty stomach with vitamin C. Avoid taking iron simultaneously with calcium, which inhibits absorption.
Fiber supplements
When dietary fiber falls short despite efforts to include fiber-rich foods, supplementation helps maintain digestive function and gut health.
Psyllium husk provides soluble fiber that softens stool and supports regularity. It also feeds beneficial gut bacteria.
Partially hydrolyzed guar gum offers prebiotic benefits with less bloating than some fiber sources.
See our detailed article on fiber and GLP-1 therapy for comprehensive guidance on types, timing, and dosing.
Electrolyte supplements
For users struggling with dehydration symptoms, muscle cramps, or fatigue despite adequate water intake, electrolyte supplementation addresses mineral imbalances.
Products like LMNT, Drip Drop, or similar formulations provide sodium, potassium, and magnesium in ratios supporting hydration. Many users find these easier to consume than plain water.
Our article on hydration and electrolytes provides detailed guidance on electrolyte balance during GLP-1 therapy.
Supplements to approach with caution
Not everything marketed to GLP-1 users deserves a place in your regimen.
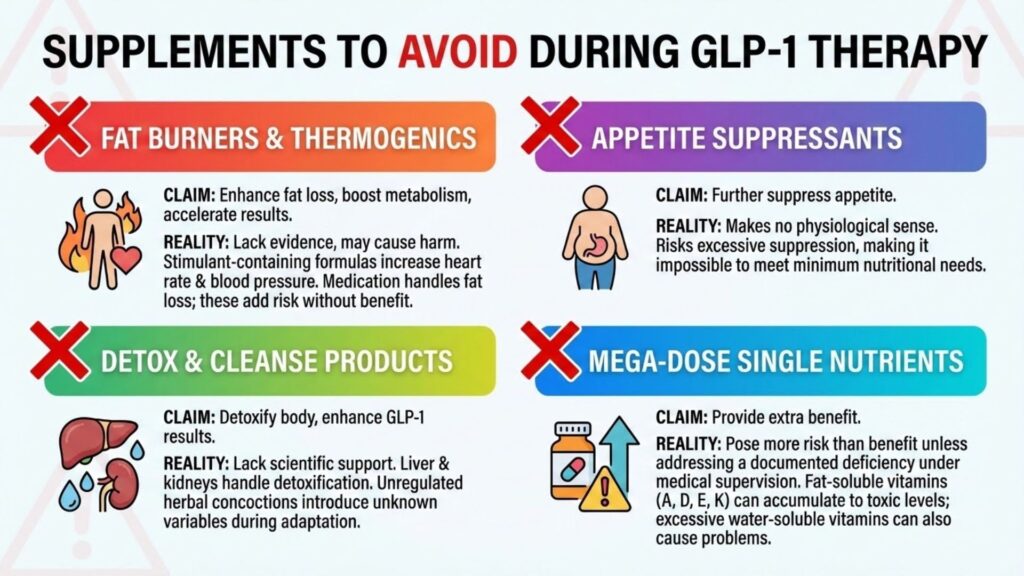
Fat burners and thermogenics
Products claiming to enhance fat loss, boost metabolism, or accelerate results alongside GLP-1 medications lack evidence and may cause harm. Stimulant-containing formulas can increase heart rate and blood pressure, concerning additions to medications that may already affect cardiovascular parameters.
Your medication handles fat loss. Additional thermogenic supplements add risk without meaningful benefit.
Appetite suppressants
Taking additional appetite suppressants alongside medications that already powerfully suppress appetite makes no physiological sense. The combination risks excessive appetite suppression that makes meeting minimum nutritional needs impossible.
Detox and cleanse products
Products claiming to detoxify your body or enhance GLP-1 results through cleanses lack scientific support. Your liver and kidneys handle detoxification. Adding unregulated herbal concoctions introduces unknown variables during a time when your body is already adapting to significant changes.
Mega-dose single nutrients
Unless addressing a documented deficiency under medical supervision, mega-doses of individual vitamins or minerals pose more risk than benefit. Fat-soluble vitamins (A, D, E, K) can accumulate to toxic levels. Even water-soluble vitamins in excessive amounts can cause problems.
Creating your supplement protocol
A reasonable supplement regimen for most GLP-1 users includes:
| Supplement | Dose | Timing |
| High-quality multivitamin | As directed | With breakfast or lunch |
| Vitamin D3 | 2,000–4,000 IU | With any meal containing fat |
| Vitamin B12 | 500–1,000 mcg | Morning, any time |
| Magnesium glycinate or citrate | 200–400 mg | Evening |
| Omega-3 fish oil | 1,000–2,000 mg EPA/DHA | With any meal |
| Protein powder | 20–40 g as needed | Between meals or post-workout |
Add situational supplements based on individual needs, symptoms, and blood work results. Remove or adjust based on how your body responds.
Working with healthcare providers
Discuss your supplement regimen with your prescribing physician or a registered dietitian experienced with GLP-1 patients. They can:
- Order baseline and follow-up blood work to identify specific deficiencies
- Recommend appropriate doses based on your individual levels
- Identify potential interactions with other medications
- Adjust recommendations based on your response to treatment
Supplements support but do not replace the foundational nutritional strategies outlined in our complete guide to GLP-1 nutrition. Protein intake, food quality, hydration, and meal timing matter more than any pill.
What supplements have made the biggest difference in how you feel during your GLP-1 treatment?